
When the pandemic first hit America, the states hardest hit were mostly “blue states” such as Washington, New York, New Jersey and Massachusetts. With the notable exception of Washington, they remain the hardest hit states in terms of cumulative deaths per capita.
A Yahoo article points out that in recent months the “red states” have been getting hit harder than the blue states. But that could reflect many factors such as behavior, weather, or a lack of previous herd immunity.
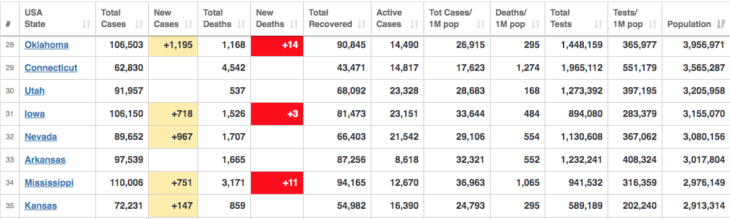
I also notice that both within the US and around the world it’s often the case that more densely populated areas have a higher rate of fatalities. This isn’t universally true (Germany has a low fatality rate) but it seems to be a strong tendency. Look at the states with the lowest rates of death per capita—most have relatively low populations:
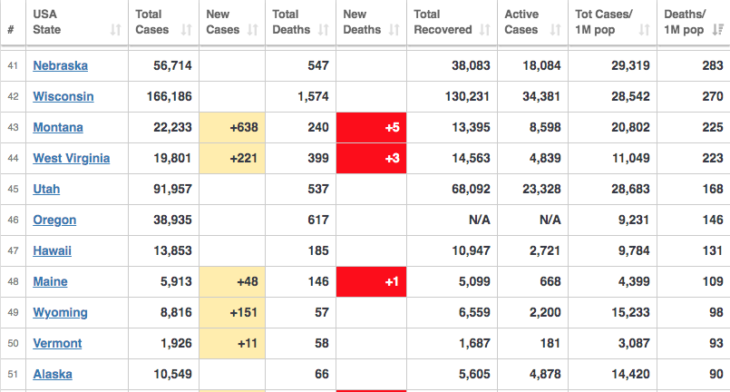
I’d like to throw out a hypothesis. Perhaps both politics and density matter. Perhaps the safest places are low-density states full of earnest do-gooders who follow public health rules. So I’m going to look at recent Covid deaths in states with fewer than 1.1 million people. Because I’m lazy I’ll take a few shortcuts, such as looking at total deaths, not per capita deaths, but that won’t affect my principle finding to any significant degree. The differences in fatalities are vast, and all these states have between a 550,000 and 1.1 million people.
I’ll first list Covid deaths since the beginning of June, and then deaths over the past two months. States will be listed from most populous to least populous:
Montana: 213/153
Delaware: 153/69
South Dakota: 245/154
North Dakota: 327/263
Alaska: 56/38
Vermont 3/0
Wyoming: 41/27
I use recent data because the initial outbreak caught many places unaware, so cultural/policy differences would have had less impact in March and April.
Vermont really jumps out, and even in per capita terms it would be an extreme outlier. This may be random, but it also might reflect the combination of really low density and “liberal” attitudes. Most low-density areas in America are red states, and Vermont might be the only strongly blue state that’s mostly rural. (Even Delaware is pretty urban by comparison.)
If you want to be safe, rent a cabin in Vermont.
This is not necessarily about politics in the normal American sense of the term. New York is left wing, but isn’t full of earnest people who always follow rules. Utah is right wing, but has a high level of civic cooperation. Utah also has a lower than average fatality rate, even relative to states with similar populations.
Germans and East Asians are known for following rules. Latin Americans are not. Notice a pattern?
PS. Let me apologize in advance for the Sumner curse, the tendency for patterns I notice to break down immediately after I post on them. Sorry Vermonters.
PPS. I was originally going to draw the line at 1 million, but Montana seems like a low-density state, despite just over a million people. On the other hand, while places like Nevada have large low-density areas, they also have major cities.
READER COMMENTS
Todd Kreider
Oct 17 2020 at 5:19pm
“(Germany has a low fatality rate) ”
Some commenting on a recent Unheard article that compares the UK with Germany state that unlike the UK, US, Sweden and many other countries, German doctors declare a Covid-19 death only for when a person dies from Covid-19 not with Covid-19 as well.
As for “following the rules,” the word “masks” was not used but implied so here are the results of a meta mask study published this May:
“In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2).”
https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
Alan Goldhammer
Oct 17 2020 at 5:42pm
The closest thing to an RCT regarding mask wearing was in Germany. Such a trial would be unethical to do given the lack of reliable therapeutics to treat COVID-19 and the need for a significant number of trial subjects. I covered this in my September 4 COVID-19 newsletter. Here is abstract & link with my commentary:
Universal masking the health care setting and in the community to contain the spread of SARS-CoV-2 has been recently recommended by the WHO, but supporting data are rare. The City of Jena was the first community in Germany to issue an order on mandatory public masking. Here, we report the development of the number of novel infections in our hospital and the city of Jena after implementation of universal masking in our hospital and the city. [note; this is from the moderately sized city of Jena in Germany who implemented a mandatory public masking law. They had a comparison city that implemented their own masking law four weeks later. Jena saw no new COVID-19 case whereas Erfurt continued to observe case until their citizens masked up. As the authors of the paper note, this is an observational study and an ethical controlled trial on mask use versus non-mask likely could not be done. I think this nice study closes out the question of whether masks work. I do not plan to cite any future papers on this topic as for me the question is settled!!! MASK UP WHEN YOU GO OUT. ‘Nuff ] https://www.medrxiv.org/content/10.1101/2020.09.02.20187021v1
Scott Sumner
Oct 17 2020 at 6:13pm
I’d encourage you not to rely on questionable sources for mortality. Germany has done very well:
https://ourworldindata.org/excess-mortality-covid
And masks certainly work, many studies show this to be true.
Todd Kreider
Oct 17 2020 at 7:16pm
Here is one quote:
Barry Wetherilt: “My understanding is that the definition of a Covid death in Germany is very different from that in the UK (and most other countries). That is, in Germany you must have actually died of Covid whereas in the UK you simply have to have tested positive within the last 28 days of dying for any reason (up to recently even longer).”
An analysis o excess deaths is important but not easy to do as Nobel laureate Michael Levitt has pointed out in his recent eight points after 2,500 hours studying this pandemic. Here are the first four:
1) Ignore cases, use number of hospitalizations, deaths.
2) Beware of reported death: many ‘with’ not ‘due to’ COVID19.
3) All-cause deaths bias-free but ambiguous & badly delayed.
4) MSM is rarely right. WHO often right but timing off.
“And masks certainly work, many studies show this to be true.”
I still find it odd that despite you repeating this statement you never seem to be able to link to a study to support this.
Scott Sumner
Oct 17 2020 at 11:04pm
If the Covid numbers and the excess death numbers are telling the same story, why would anyone rely on an anecdote from some doctor in Germany?
And it’s not just that they tell the same story for the year as a whole, they line up pretty closely month to month. Both tend to spike in March and April. You really need to believe the errors in BOTH data sets were extremely large to argue that Germany doesn’t have a vastly lower Covid fatality rate.
I’ve linked to studies of masks in previous posts; you can easily google such studies if you are interested. If they don’t work then someone should tell doctors so that they don’t have to bother wearing them any longer in hospitals.
Todd Kreider
Oct 18 2020 at 2:38am
Scott,
I’ll answer your question when you explain why you deleted my comment:
Benoit Essiambre: Note the word “significant” has a very specific meaning in statistics that does not mean there is no effect. This experiment was consistent with a 49% reduction or a 20% increase in transmission from masks, “CI 0.51–1.20”. All “not significant” tells you is that this particular experiment’s data was too noisy to tell anything.
me: This isn’t correct. Here is part of the abstract:
Although mechanistic studies support the potential effect of hand hygiene or face masks, evidence from 14 randomized controlled trials of these measures did not support a substantial effect on transmission of laboratory-confirmed influenza.
Amy Willis
Oct 18 2020 at 11:06am
Todd, your comments were not deleted, merely held in our spam filter. When you submit a large number of comments at near the same time, the filter will (rightly) flag it. Trying again will only trigger the filter. Thanks for your patience.
john hare
Oct 18 2020 at 5:41am
There is a vast difference between trained professionals using masks properly and an uncaring public being forced to wear something resembling masks. The vast majority of “masks” I see in public are not used anywhere near correctly and are certainly not the pro grade equipment used by doctors.
Under the right conditions masks work. Under the conditions I see on a daily basis, they can’t. And under some conditions, they are actually worse than nothing, such as when kept in a pocket and used a few times a day for weeks without washing or replacing.
In construction, it is generally understood that PPE only works when used right under the proper conditions. It is understood to be safety theater otherwise. A mask properly used by a thinking individual that understands the limitations is not what I see around my area.
Scott Sumner
Oct 18 2020 at 9:31am
John, Your claims have been tested and found to be incorrect. Actual use of masks by the public during Covid-19 has reduced transmission.
Todd Kreider
Oct 18 2020 at 12:01pm
Scott, you have not linked to the studies whereas I linked to the meta study and the 2015 Australia/Vietnam random controlled study that showed health care workers in six hospitals in Vietnam who wore cloth masks had contracted significantly more viruses than those who did not wear masks. The authors stated that cloth masks had a 97% penetration of virus whereas medical masks had a 44% penetration and that:
“Although efficacy for medical masks was not shown, efficacy of a magnitude that was too small to be detected is possible.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4420971/
As Michael Levitt points out, getting information from excess deaths is tricky. At the Unherd article, three people wrote that Germany is counting only deaths from Covid-19 and not with Covid-19. Why does Poland have even fewer Covd19 deaths than Germany? Did they “do even better”? (Japan has 15 times fewer deaths than Germany. Did they really “do even better”?) The assumption that all countries started with the same initial conditions and are counting deaths the same way is false. Even Scotland was counting Covid deaths differently from England and Wales until mid July when Scotland’s counting by limiting deaths to dying within 28 days after a positive test revealed coronavirus was better than keeping it open ended and as a result, Covid deaths went down in the UK by about 5,000.
Scott Sumner
Oct 18 2020 at 2:55pm
Todd, I’d encourage you to be more careful when evaluating evidence. I believe you tend to jump to conclusions on very limited evidence. To answer your question, I’ve never once deleted a comment on Econlog.
JFA
Oct 18 2020 at 8:11pm
Germany has done very well, but the excess deaths for Germany was at 17,800 through Sept 24 (https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938). The official tally of Covid deaths for Germany was about 9500. I’m guessing they are undercounting Covid deaths quite a bit. They are still doing well even if all the excess deaths are from Covid, just not as well as the Covid count suggests.
Todd Kreider
Oct 19 2020 at 3:31pm
But why are German doctors necessarily undercounting Covid deaths if they chose to count only deaths from Covid and not “happen to also have” Covid. (There can be unclear cases, of course.) There is still this notion that governments have control over a pandemic so that “Japan did great!” despite a lot of criticism in March and early April. How could the Japanese government not be credited for brilliant policies when per capita deaths are 55 times lower than the U.S., the U.K., Sweden and Italy; 40 times fewer Covid 19 deaths than France and 10 times fewer Covid deaths than Germany – “the country that has done very well”? All of these countries had different initial conditions.
JFA
Oct 20 2020 at 10:04am
I think Japan (as a country) has done pretty well (I also think that there have been mutations in the virus that made the European and US east coast experiences much worse than in east Asian), but they also speak softly and wear masks when sick as cultural norm. I’ll address your question about the death certificates, because there is a dangerous obstinance in some circles to downplay the number of deaths caused by Covid (recognizing reality doesn’t necessitate that you accept certainty policy decisions, but it does help make you not seem like a kook).
During the AIDS crisis in the early 1980s, doctors noticed that there were many more deaths caused by Pneumocystis carinii pneumonia (PCP) (a rare-ish type of pneumonia) than usual. Before HIV/AIDS was finally identified as an infection, PCP and other infections were listed on the death certificates of those who died. Now, would we say that those who died of PCP did not also die because of AIDS? I don’t think so. We recognize that there can be multiple complicating factors that lead to someone’s death.
So now we come to the Covid pandemic. For some reason, there is an enormous amount of excess deaths around the world (in the US, we are on track to increase the number of deaths this year by more than 10% over the average of the past few years). A few of these death certificates list only Covid-19 as a cause of death, while most other death certificates list other diseases along with Covid. Are we then to conclude that during a pandemic that there is also just a surge of deaths caused by, for example, diabetes (~11,000 deaths above the 2015-2019 average), various circulatory diseases (~44,000 deaths above the 2015-2019 average), and Alzheimer and dementia (~31,000 deaths above the 2015-2019 average) (https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm). Are we to believe that Covid has nothing to do with any of those deaths? A person can live with hypertension and diabetes for a while. If some serious illness comes along and weakens their body’s ability to deal with those comorbidities, is it so crazy to suggest that absent that serious illness, the person might have continued living? If that is the case, is it that unreasonable to claim that the serious illness could be consider the cause (or at the very least, a cause) of death?
Here’s another question for everyone pushing the line that many Covid deaths are those “with” other diseases and those deaths shouldn’t be counted as Covid deaths: doesn’t this also go the other way? Aren’t those extra heart disease and diabetes deaths also listed “with” Covid? Why should we list those deaths as caused by heart disease or diabetes and not Covid? Wouldn’t that be over-counting heart disease and diabetes deaths? Once you realize that that is a moronic question and that there can be multiple causes of death, you’ll realize how most thinking people view the claim that Covid deaths are being over-counted based solely on the fact that there are multiple comorbidities listed on the death certificate.
mark
Oct 20 2020 at 9:53am
Nein. Nicht korrekt, total falsch. German here. Deaths of ALL who are covid-positive are counted as “Covid-deaths” in Germany. (as most anywhere – though it seems Belgium even counts those who are believed to have been positive, or so.) – Which obviously leads to some over-counting (the 94 year old lady who was the most recent case in my hometown might have died of anything, of course. Only autopsies can clear that; they are done mostly in Hamburg by outstanding Prof. Püschel – he found in all Hamburg cases serious other health-defects and in a few cases deaths completly unrelated to Covid. They are still counted as Covid-deaths.) So there is over-reporting – but then there are “enough” deaths by untested/unreported to compensate for this. In all: hardly any over-mortality in Germany. Mask-wearing-compliance is at about 95% in most places (shops, buses, …) . Arabic barber-shops: 30%. Restaurants with over 200 guests: 1% – as it is not required at the table. (As I lost my teaching-job due to Covid, I do mask-control-tours for my town.)
Todd Kreider
Oct 20 2020 at 4:08pm
Japanese speak softly and wear masks (both irrelevant) so their Covid-19 death count is 60 times lower than the U.S. and most of Western Europe? That is having “done pretty well”? So far there is no evidence that the coronavirus that entered Japan and South Korea was any weaker than the virus that entered the West at the same time. When controlling for various factors it has been shown that Japanese wearing masks have the same per capita deaths as Germans who do not wear masks. Why would we expect masks to suddenly offer notable protection with Covid-19?
In May, the Colorado government said that it had over counted Covid-19 deaths by 24% since those deaths were clearly not Covid-19 related. The U.K. didn’t do a similar review but did reduce its Covid-19 deaths by 10% in July as it decided Scotland’s approach to limit Covid-19 deaths to within 28 days of testing positive instead of having no limit.
By the way, Nobel laurate Michael Levitt recently calculated that there have been 32% more Covid-19 deaths in the EU than there were influenza deaths in Europe in 2017/2018 over comperable 24 week periods.
https://twitter.com/MLevitt_NP2013/status/1317815299454857217?s=20
JFA
Oct 20 2020 at 8:45pm
I know you meant to reply to me, but we’ll continue here. Since you didn’t address my point about how deaths are counted, I just want to reiterate that a person’s death can be caused by multiple things. A death certificate listing Covid “with” other causes does not mean Covid wasn’t a factor in the death.
Here is evidence for different strains affecting transmissibility: https://www.biorxiv.org/content/10.1101/2020.04.29.069054v2, https://www.biorxiv.org/content/10.1101/2020.06.12.148726v1, https://www.cell.com/cell/fulltext/S0092-8674(20)30820-5?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0092867420308205%3Fshowall%3Dtrue. TL;DR: the strain more dominant in Europe and the east coast of the US spreads much more efficiently than the strain dominant in east Asian. If it spreads less efficiently, there will obviously be fewer deaths.
Speaking more softly spreads virus less (that’s why choirs were superspreader events) and face masks block droplet exhalation that might contain the virus. Couple those with a virus that spreads less efficiently, you get fewer deaths.
I am perfectly willing to entertain other factors such as prevalence of certain blood types, differences in genetics, etc. But policy (and cultural practices) probably has something to do with it, otherwise you wouldn’t have maps that look like this one: https://twitter.com/MaxCRoser/status/1317226352161017857?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1317226352161017857%7Ctwgr%5Eshare_3%2Ccontainerclick_1&ref_url=https%3A%2F%2Fwww.vox.com%2F21514530%2Feurope-covid-second-wave-update.
“When controlling for various factors it has been shown that Japanese wearing masks have the same per capita deaths as Germans who do not wear masks.” Citation please.
Current Covid deaths for UK is ~43,000. Current excess deaths over recent years is ~67,000. UK probably not undercounting Covid deaths. Their approximation method for including deaths within 60 days of diagnosis was a bit odd, and the 28 day rule is I think a decent one for approximating potential Covid deaths.
Colorado made a change in how data are input on May 15 (or so). Okay? About half the Covid deaths in Colorado have occurred since then. And you seem to think mismeasurement only goes one way. Why?
I don’t really understand your last point. Isn’t that just another way of saying Covid is more deadly than the flu? Is this the dry tender hypothesis, where the weak weren’t culled by earlier flu and so Covid is having a field day… maybe. Doesn’t really explain the US, though. The 2017-2018 flu was “bad” which means about ~15,000 excess deaths. The 2016-2017, 2018-2019, and 2019-2020 were not super severe, so maybe there was some dry tender for Covid to burn through. Extrapolating from the 2017-2018, that might account for some of the excess deaths, but I’d have to do a more analysis. But now your story is getting complicated: deaths are being way overcounted and Covid is killing way more people than we would expect because the flu didn’t kill them.
By the way, flu deaths for 2020 are higher than the average of the past few years.
MarkW
Oct 17 2020 at 5:35pm
If you want to be safe, rent a cabin in Vermont.
Rent a cabin in virtually any rural location and don’t spend time inside restaurants and bars. For a bit of (probably unnecessary) extra safety don’t hike crowded trails. Your chance of contracting the virus is essentially zero regardless of what the non-strictly-rule-following locals may be up to. When we’re at our cottage in northern Michigan (in a Trump-leaning area), the virus might as well not exist other than during infrequent trips to the grocery store (the county of ~20,000 has had under 100 total cases and 2 deaths since the beginning of the pandemic). And that’s despite the fact that it’s home to beaches, tourist towns, golf courses, resorts, and popular National Park that’s been even busier than usual this year (with more people favoring outdoor activities and destinations within driving distance). The county’s death rate would put it on par with Vermont, Wyoming, Maine, and Alaska at around 100 per 1M. Bottom line — go to a low-density area and you can occupy a space that’s as safe as you want it to be.
Scott Sumner
Oct 17 2020 at 6:15pm
I agree, but your comment relates to my throwaway joke, not the substance of my post. The biggest towns in Vermont are similar in size to the biggest towns in places like Montana.
MarkW
Oct 19 2020 at 8:01am
But the throwaway joke matters, I think. There seems to be a widespread belief that one’s personal safety is dependent on rule following by others living around you. That’s largely true in high-density areas. When you live in an apartment, rely on public transport, buy groceries in small urban stores and have to navigate down crowded sidewalks and park paths (much more crowded now that gyms and subways are lightly used), then general compliance matters. My daughter, who lives in Chicago (another lefty but non-rule following city) has taken up walking in a large cemetery in her neighborhood.
But when you live in a detached house, get around by car, have ready access to uncrowded outdoor areas, and shop in big box grocery stores, your risk and exposure is largely dependent on your own family’s behavior and nobody else’s (do you go to parties inside friends’ houses? Do you go to bars?) And because the virus ‘velocity’ is much lower, even those potentially risky behaviors are safer in low density areas.
So sure, politics and density both matter. And culture, too, of course (is it taboo to mention this?) — some ethnic groups are used to frequent large family gatherings and seem not to have entirely given them up. And these folks tend to live in urban areas — a double whammy for a pandemic. But I think the numbers show that density matters the most. And outside high-density areas, while politics and culture still affect overall numbers, they have little effect on your own safety.
And BTW, has anybody else noticed the inevitable Peltzman effect with mask wearing has started to kick in? I’ve across quite a few now who seem to think that because they’re wearing a mask, maintaining a distance is no longer needed.
Benoit Essiambre
Oct 17 2020 at 6:03pm
Note the word “significant” has a very specific meaning in statistics that does not mean there is no effect. This experiment was consistent with a 49% reduction or a 20% increase in transmission from masks, “CI 0.51–1.20”. All “not significant” tells you is that this particular experiment’s data was too noisy to tell anything.
Todd Kreider
Oct 17 2020 at 6:55pm
They aren’t discussing statistical significance there. Here is part of the abstract:
“Although mechanistic studies support the potential effect of hand hygiene or face masks, evidence from 14 randomized controlled trials of these measures did not support a substantial effect on transmission of laboratory-confirmed influenza.”
Scott Sumner
Oct 18 2020 at 2:56pm
Absence of evidence is not evidence of absence.
Mark Z
Oct 18 2020 at 3:31pm
This probably doesn’t change much, but fraction of people living in urban areas or density of urban areas probably matters more than population density per se. States whose populations are concentrated in dense metropolises will not be helped much just by having vast, adjacent, sparsely populated territories (e.g., upstate New York, all the wilderness in California).
IVV
Oct 19 2020 at 3:01pm
True, and we see this effect in Spain.
Spain has an overall low population density, but the population itself is mainly densely packed in cities, like Madrid and Barcelona. So covid was/is rampant in Spain, even though the density for the country as a whole is low.
Michael Pettengill
Oct 19 2020 at 5:31am
The initial outbreaks were started by travelers from Europe. The focus on China distracted from the real threat in a global economy.
Knut P. Heen
Oct 19 2020 at 12:04pm
I think the virus spreads like Brownian motion (like heat). People randomly bump into and infect each other. If no one takes a random trip to village X, no one in village X will be infected. But if someone in village X becomes infected, it may spread quickly in the village if the villagers interact a lot with each other.
A village of two persons is not very likely to get the virus, but if one person gets it, the village may quickly reach 100 percent. We therefore expect to see rural places at the top and bottom of these lists. Rural places also tend to have a high fraction of elderly people (except places like Utah with a high birth rate) . I thus expect to see some bad mortality statistics once the virus really hits these places.
Comments are closed.