
It might seem surprising to find a defense of Euro-style health care in a market friendly blog. In fact, I actually prefer the small government approach of Singapore to either the European or the US system. Nonetheless, I’m going to argue that the European system (or systems) is probably better than the US system.
But I won’t stop there. I also argue that (despite their claims) American progressives do not favor anything even close to the European system, and indeed that I am just about the only America pundit who actually advocates that we adopt the European system.
Under my “Medicare for all” system, the Medicare program would be provided with funds equal to 8% of GDP, and then instructed to provide as much health care as possible to all 325 million Americans. If the funds were not sufficient, they’d be rationed on the basis of need, with broken legs being treated before things like hip replacements. (Sorry mom!)
Those who are not satisfied with the healthcare provided by “Medicare for all” would be free to buy additional care in the private market. To better understand this system, consider this graph of health care spending as a share of GDP:
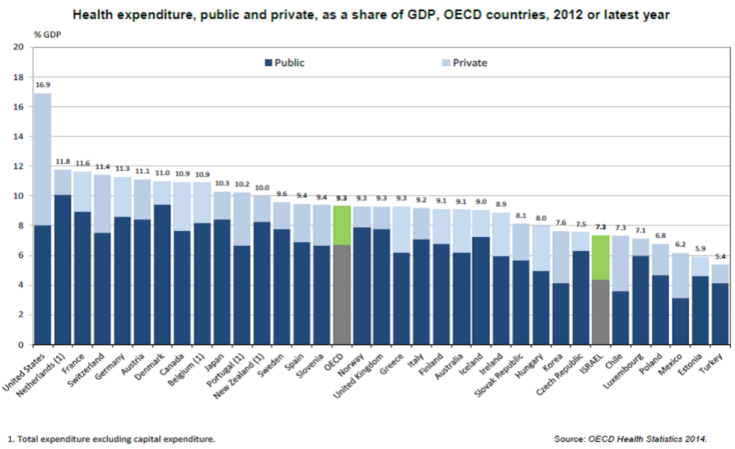 As you can see, the US spends nearly 17% of GDP on health care, of which 8% is spend by the government. The 8% figure is above average for OECD countries, and indeed is higher than public spending on health care in places like Sweden, Canada, UK, and even oil rich Norway. But it gets even better. Not only would my program have the US government spend an above average share of GDP on health care, but US per capita GDP is also well above the OECD average. Thus under my plan, total per capita public spending on health care would be 30% to 40% above the OECD average, which is far more than enough extra money to cover the higher drug prices in America, and continue to spur new drug innovation (if that’s your concern.)
As you can see, the US spends nearly 17% of GDP on health care, of which 8% is spend by the government. The 8% figure is above average for OECD countries, and indeed is higher than public spending on health care in places like Sweden, Canada, UK, and even oil rich Norway. But it gets even better. Not only would my program have the US government spend an above average share of GDP on health care, but US per capita GDP is also well above the OECD average. Thus under my plan, total per capita public spending on health care would be 30% to 40% above the OECD average, which is far more than enough extra money to cover the higher drug prices in America, and continue to spur new drug innovation (if that’s your concern.)
Under my plan, the government would no longer subsidize private health care spending, and since everyone would be covered by “Medicare for all”, I’d anticipate that private spending would fall sharply as a share of GDP, perhaps from 9% to 2% or 3% (as in Europe). That would provide a huge boost to American living standards.
You might wonder whether there is a downside to my plan. No, there is not.
If we tried to cover all Americans with spending that now covers the old, poor, veterans and government employees, would quality suffer? I believe it would suffer, but only a tiny bit. And I’ll argue that the reduction in quality is probably trivial relative to the cost saving. In other words, the 8% of GDP that we now spend providing health care for a modest fraction of Americans involves massive waste (as does the heavily subsidized “private” insurance system.) My plan is better on both equity and efficiency grounds.
Is there evidence that American health care is better than European health care? I know of two arguments for that claim, neither of which seem very important to me:
1. American health care is certainly more luxurious. I immediately noticed this when I went to the doctor in London in 1986. But I’ve also read that other European countries like France have higher quality than the UK (which itself has improved since 1986), so I don’t know how big the difference is today.
2. Cancer survival rates are modestly longer in the US. Assuming this is not just earlier diagnosis of cancer, you have to ask whether extremely expensive treatments that produce a few extra months of suffering with painful cancer passes the cost/benefit test.
Most importantly, under my plan even those with a stronger desire than me to “hang on for dear life” with terminal cancer, would have the option to spend extra private money on treatment. So I am still providing a sort of market safety valve. If you think I’m wrong about heroic treatments, feel free to spend the extra money yourself.
There are other arguments that make me convinced that the US system is highly wasteful:
1. There are no market controls on excess spending. All the incentives in the system are in the direction of providing excessive services, at excessive costs.
2. Whenever people I know interact with our health care system, I see enormous waste. I won’t bore you with the details, but I firmly believe that more than 50% of the funds I’ve seen spent on me or people I know have been completely wasted. Without any market test in the other direction, I’m going to assume the system is very wasteful. When you are spending 8% of GDP, the burden of proof is on those who claim effectiveness, not those who are skeptical. And if the European system really were greatly deficient, and the extra spending here was worth the cost, surely the proponents of our system would be able to come up with anecdotes more persuasive than modestly longer cancer survival rates.
Another question is how we get from here to there. There is only one realistic answer—gradually. But that’s going to be true of any alternative reform, as Congress is reluctant to take dramatic steps. I’d tell the Democrats that if they want the European system, then implement the European system. Gradually squeeze costs, and use the cost savings to gradually expand coverage of Medicaid. The European system does not have the government spend 17% of GDP on health care. I get angry when progressives say that Europe shows “Medicare for all” can work. It shows that a program spending 8% of GDP on health care can work; no one has ever been able to show a government program spending 17% of GDP on health care can work, indeed no one has ever tried. I doubt whether a European country could implement such a program without going bankrupt. Indeed Greece has already gone bankrupt and Italy is teetering on the edge, despite their government’s spending only 6% to 7% of GDP on health care—even less than the US.
The progressive call for the US to adopt a European style health care system is profoundly dishonest. If they really believed in such a system, they would extend existing government health care to all 325 million Americans, without spending additional money. That’s the European system. But that’s not what they are proposing.
The GOP position on health care is equally dishonest. Recall when people started showing up at Tea Party rallies with signs for the “government” to keep their hands off the Medicare program.
Our current GOP president has promised to protect this wonderful program. Well if Medicare is indeed a wonderful program, then why shouldn’t all 325 million American benefit from the program? Why do only the old, poor, military and public employees get government health insurance?
Even worse, not only did the GOP renege on its promise to repeal Obamacare, but voters in deep red states now seem supportive of expanding Obamacare to even more people:
Gooding is a small town in Idaho, one of America’s most conservative states. It is the sort of place where a campaigner may encounter a man butchering an elk on the dining-room table. It is not a place where you would expect to find much support for a ballot initiative that would expand Medicaid, the government health-insurance programme for the poor. Medicaid expansion, after all, is a pillar of the Affordable Care Act, as Obamacare is formally known. Yet Molly Page, an organiser, gets a surprisingly kind hearing from local people.
One woman turns out to be a fervent supporter of President Donald Trump who fears a deep-state conspiracy to remove him from office. She nonetheless supports the ballot measure. Her two adult sons are uninsured, including one with alcoholism and epilepsy who skipped treatment because “it’s too damned expensive”. Even the elk-butcherer, a few doors away, hears Ms Page out. Polls suggest that a comfortable majority of Idaho’s voters will approve Medicaid expansion on November 6th. Voters in Utah, Nebraska and Montana will probably do the same.
If you listened to the GOP small government rhetoric, you’d think they’d support my plan to cap public spending on health care at 8% of GDP. Instead everyone from red state voters to the President are pushing to expand the footprint of the government. “Protecting Medicare” is a code word for expanding Medicare. Medicaid is also likely to grow, pushing government health care spending well above 8% of GDP, while leaving millions uninsured.
The sad truth is that neither party is committed to the European system, and hence my proposal will fail. But here’s what else will fail. The dreams of both progressive and libertarian pundits are every bit as politically infeasible as my proposal, at least in the short run. We are not getting Medicare for all (as progressives prefer), and we are not about to get the (small government) Singapore health care system, where public spending on health care is only 2% of GDP.
Sad.
PS. At MoneyIllusion I have a new post discussing my new economics principles textbook. If you are a principles instructor, please check it out.
READER COMMENTS
roundtree
Oct 31 2018 at 3:47pm
There’s certainly an elegance to the system that you outline, but there’s one large difference between the few European systems that I don’t see mentioned: systems like the UK NHS are centralized, nationalized systems; systems like those used in Denmark and Sweden are far more decentralized and, as such, put the tax burden/care spending mostly at the local level. There’s little question that most progressives are arguing for the former, not the latter.
OTOH, I struggle to see how the Singapore system would differ greatly in the US, since it would need to scale in some manner, whether through a centralized or decentralized approach. I’m very certain that there are concepts like their Medisave that could be married to the distributed Scandanavian model to get a best of both worlds and keep market forces in charge instead of bureaucrats.
jj
Oct 31 2018 at 4:44pm
Sadly, your proposal will fail on political grounds. One reason that Europe and Canada get by with only 8% spending is that the governments set the payment rates for health care. In the US, the side effect of setting low Medicare payment rates is that many doctors refuse to accept Medicare patients. The obvious progressive solution will be to ban private health care so that doctors have no choice! And that’s how Canada ended up disallowing private health care from covering anything that is covered by public health care. The few % of private spending is for non-covered areas like drugs, medical devices, dentistry, and whatever else the OECD defines as “health expenditure”.
Scott Sumner
Oct 31 2018 at 5:21pm
You said:
“Sadly, your proposal will fail on political grounds.”
I agree, but I still think it’s better than our current system.
Jan Haugen
Nov 2 2018 at 1:22pm
Health care economists sometimes recommend the systems of Germany and Switzerland because there is a major role for private insurance there. Its though t that that would reduce the political barriers a little.
Those systems are a bit more expensive than the European norm but also tend to do well in responsiveness.
bob
Nov 1 2018 at 11:41am
I don’t think you would need to ban private insurance. There would be doctors who only take private insurance, but most doctors would not be able to attract enough patients to be able to refuse medicaid. We could also reduce the barriers of entry into the profession if it really became a problem. There are plenty of qualified doctors in Europe and other advanced countries who could immigrate here. Or medical schools could accept more students. I don’t think that would be necessary. I expect it would be similar to the market for therapists in which many therapist refuse to accept insurance because the rates are low, but there is no shortage of therapists who do accept health insurance, because they don’t have a choice. US doctors make significantly more than doctors in other countries. It’s not just drub prices. Scott’s plan is a great plan. I would go with 10%, because trying to get to 8% would be too disruptive, and it makes sense that a rich country like the US would use to spend a larger share on health care, now that everyone has a smart phone and a flat screen.
Jan Haugen
Nov 2 2018 at 1:20pm
Governments don’t really set the pay raters in any western nation I know. What they do is use their market power as by far the biggest customer to negotiate prices. Thats not really the same thing.
Peter Raasch
Oct 31 2018 at 4:54pm
Whats the basis for calling Singapore’s healthcare “small government”? Reading this it seems completely government controlled? http://assets.ce.columbia.edu/pdf/actu/actu-singapore.pdf
Seems like this is one of the standout factors: ” Under a scheme without risk pooling, individuals have to be responsible for their own costs”.
Even in completely voluntary systems you would find some risk pooling, wouldn’t you (examples on a local level certainly exist). State enforced individualism, that’s new =D
pyroseed13
Oct 31 2018 at 5:23pm
This is a good post Scott. Are you familiar with Larry Kotlikoff’s Purple Plan? It’s basically “Medicare Advantage-for-all” and similar to your proposal here.
Scott Sumner
Oct 31 2018 at 5:25pm
Not familiar with it. Does it cap spending at 8% of GDP?
pyroseed13
Nov 1 2018 at 8:39am
I believe it caps it at 10%.
Scott Sumner
Oct 31 2018 at 5:24pm
Peter, Yes, they have a lot of government intervention in health care, but far less than the US or Europe. And they have some market-oriented features, such as HSAs.
robc
Nov 1 2018 at 4:32pm
Hmmm…this made me wonder.
How about instead of your plan, we eliminate government spending on health care (directly) and put 8% of GDP into HSAs, split evenly between every US citizen?
If I calculated correctly, that is about $4800 per person.
derek
Nov 5 2018 at 9:24am
Because most people will not come close to using that much money on health care, but some people, because they have the misfortune of getting in horrible car crashes, contracting diseases, inheriting expensive medical conditions, etc., will need far more. Just because Scott proposes switching away from private insurance does not mean we do not need a mechanism for risk pooling.
Floccina
Oct 31 2018 at 5:25pm
Great post!
Ever since I listened to Robin Hanson in this podcast I’ve being asking my Democrat friends who like to laud European healthcare, to push for covering everyone for what Government spends now. It seems that the margin healthcare dollar does not improve health significantly so the downside should be small.
Start by having medicare refuse to pay for some of the least effect care (Ive read that heart bypass is rarely done and shows little positive effect of health above much cheaper treatments.) Then have medicare try to negotiate lower prices.
But IMO they made a big mistake covering the old first. The old vote. And Healthcare for the elder;y is generally much less effective than for the young.
Also it seems to me that much of the problem with cost is at the state level where most medical regulation is made. AZ and UT seems to do OK. The bigger the part of Healthcare paid for by the Fed Gov. the less the incentive for state regulars to regulate with cost in mind. Perhaps the Fed Gov should give the money to the states on on an age adjusted per capita basis and say to the state you much at least cover those over 65.
nobody.really
Oct 31 2018 at 5:54pm
All 325 of us, huh? We wouldn’t even make up a strong cheering section at a college football game, but at least we’d have health care….
I had never really thought about this before: Is health care part of compensation packages in Europe? For example, the European nations offer heath care benefits to veterans that differ from the benefits available to citizens at large? (I expect the answer may differ for different nations.)
An EXPLICIT link to 8% of GDP would be interesting. Today Democrats want to push back on Trump’s tax cuts because the benefits flow disproportionately to the rich, and the resulting stimulus is not covering the resulting costs. But an 8% link would give Democrats a greater incentive to drive up GDP, even with its skewed distribution. (Then we’d have nobody objecting to deficits; yippee….)
I’m curious how European systems operate with this finite compensation rule. Each year the national health service announces which kinds of services they’re covering? And private providers then leap into or out of given markets, given what the local authorities have announced? For example, a private hospital might build a maternity ward and higher staff for this year, and then lay off the staff and close the maternity ward the following year? I’m skeptical.
Scott Sumner
Oct 31 2018 at 6:57pm
Thanks for pointing out the typo. The Europeans engage in rationing of health care. Think of it this way. Suppose the US government had a program giving a free car to everyone. Most people were asking for luxury cars. Then I came along and suggested that everyone get a $20,000 car at most, and if they don’t like it then buy another car with their own money. Isn’t my program less bad than giving everyone whatever car they wanted? Isn’t it cheaper?
nobody.really
Nov 1 2018 at 9:21am
Oh, I get the theoretical advantages of capping expenditures. I’m just curious about how it works in practice. Does the list of covered services actually fluctuate year to year? Is the coverage for citizens in general really equal to the coverage for veterans, or the elderly, or public employees? That sort of thing.
Hazel Meade
Nov 1 2018 at 1:29pm
Would you be ok with people taking the $20,000 care, selling it, and then spending the $20K on a better one?
Ahmed Fares
Oct 31 2018 at 8:11pm
Speaking as a Canadian with single-payer healthcare, it’s important to ban private healthcare.
One of the reasons is:
“Efforts to attract Doctors and other staff to private clinics can often drain needed resources from the public sector.”
The above quote is from here: http://www.friendsofmedicare.org/privatization
Also, it’s important to keep rich people in the system so as have skin in the game and not neglect the public system.
BC
Oct 31 2018 at 8:47pm
“Those who are not satisfied with the healthcare provided by ‘Medicare for all’ would be free to buy additional care in the private market.”
Is that really a feature of European systems? I thought that the Charlie Gard and Alfie Evans cases were about people not being able to spend their own (or private donors’) money for additional health care.
I would certainly agree to limiting government spending on healthcare to 8% of GDP and allowing that money to be spent on everyone (not just seniors, the poor, veterans, etc.) if progressives in return would guarantee that anyone unsatisfied with government healthcare would be free to buy additional care privately. Such private healthcare freedom would necessarily include no price limits (on private healthcare; government could, of course, limit the prices government was willing to pay) and no limits on providers in providing private health care.
As we can see from comments above, though, progressives would vehemently object to private health care, even after getting Medicare for all (government healthcare expanded to everyone). What progressives really seem to want is private healthcare for no one.
BC
Oct 31 2018 at 9:01pm
I should also point out the irony of starting with a declaration that “healthcare is a right” and ending with government prohibition of private healthcare, as in Canada apparently. By that understanding of “rights”, the right to free speech would mean the government would pay for you to say what the government wants you to say but would prohibit you from disseminating your own speech. Disseminating your own speech would “drain resources” away from “free” government speech.
Scott Sumner
Nov 1 2018 at 1:20am
BC, I know that Switzerland is widely regarded as one of the best European systems, and they allow private healthcare. I’m not an expert on all of the different systems, perhaps someone else knows more.
Alan Goldhammer
Nov 1 2018 at 9:02am
Best starting place to compare various national approaches to healthcare is former Washington Post international correspondent TR Reid’s very readable book, “The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care.” On can easily read it in an afternoon, and Reid and his family had actual experience with foreign healthcare systems when he was posted abroad. While the book was written a decade ago, most of the foreign health care systems he writes about have not changed much if at all.
It’s also important to note that some countries have relied on the insurance model to provide universal care (The Netherlands, Switzerland, Germany) while others such as the UK rely on a central control model. Back in 2008 when I was still working at PhRMA I invited Zeke Emanuel down to give a talk on the proposal that he and health economist Victor Fuchs developed for a voucher system that would provide coverage to everyone in the US. Medicare and Medicaid would be eliminated as the voucher paid for insurance would cover all. Robert Frank has archived a copy of the original New England Journal of Medicine article outlining the proposal.
I would note that I’ve been following this issue ever since Paul Elwood convened the original Jackson Hole meetings on healthcare. Ultimately, the country will move to some form of ‘national’ healthcare. The timing of this and form are still unknown but the Affordable Care Act (AKA ‘Obamacare’) was nothing more than a kludge, designed to help a limited number of people (I’ve had first hand experience with it, helping my two daughters purchase policies when they were working as independent contractors).
Hazel Meade
Nov 1 2018 at 1:07pm
I looked into this recently.
The thing is that while technially legal, Canada imposes various regulations to effectively prevent private health care from competing with the public system. For instance, doctors may not treat both public and private patients, they much be exclusively private if they want to offer private health care.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC80881/
Our survey revealed multiple layers of regulation that seem to have as their primary objective preventing the public sector from subsidizing the private sector, as opposed to rendering privately funded practice illegal. Private insurance for medically necessary hospital and physician services is illegal in only 6 of the 10 provinces. Nonetheless, a significant private sector has not developed in any of the 4 provinces that do permit private insurance coverage. The absence of a significant private sector is probably best explained by the prohibitions on the subsidy of private practice by public plans, measures that prevent physicians from topping up their public sector incomes with private fees.
Hazel Meade
Nov 1 2018 at 1:33pm
I should say technically legal, in some provinces. It is explicitly illegal to privately offer anything covered by the public sector in 6 out of 10 provinces.
(And as noted, it is strongly disincentivized via various regulations in the other 4.)
Jan Haugen
Nov 2 2018 at 1:42pm
Yes, private healthcare is a feature of the European healthcare systems. Canada is a bit of an outlier on the subject. The amount of use varies. Switzerland I think has a for-profit insurance based system. France a hybrid system. Norway has a NHS style system but where the government puts batches of surgeries out to tender, private and public hospitals bid on them and patients pick their own hospitals to be treated at. (Obv. not for emergencies). The UK has private healthcare along with public. Americans have been known to pay privately at UK hospitals because its much cheaper than the US ones.
The Charlie Gard and Alfie Evans cases were not about funding of which there was plenty. It was about whether further treatment had so little chance (as in zero) of helping that it did not justify the suffering inflicted on the children. The parents were too desperate for any fragment of a chance, and the court cases were about when you say: “Stop, it is just pointless pain for baby now.”
gmm
Oct 31 2018 at 11:07pm
Super informative post. Thanks.
Sebastian H
Nov 1 2018 at 1:27am
Yes, the truly shocking thing about US health care is that the government spends as much per capita on health care as most of the rest of the world and only covers Medicare and Medicaid patients (and some Veterans). Additionally, the private insurance companies spend as much per capita on health care as most of the rest of the world and cover only a portion of the non-Medicare/non-Medicaid patients (and some veterans).
Worse still government spending PLUS private spending STILL doesn’t cover the whole population, while for most other countries our government spending OR our private spending is enough to cover everyone.
ARGH.
Duncan Earley
Nov 1 2018 at 1:31am
You just described the health care system in Australia …where I live 🙂
RPLong
Nov 1 2018 at 9:31am
This is the classic government health economist move. First, assume a given expenditure is wasteful; then, cut the expenditure; finally, claim 100% of the difference as “savings.”
You ought to first establish that the money Americans are voluntarily spending on health care is wasteful. Merely comparing shares of GDP to European nations doesn’t do that work for you. You’d have to first establish that Europeans wouldn’t rather spend more on health care if they didn’t have to worry about spending on things like high food prices and VATs. In general, people spend more on health care the wealthier they get. They even spend more on veterinary medicine the wealthier they get. Health care is something human beings like to buy. Just because spending levels are higher in one country than another does not mean that the difference is wasteful spending.
You don’t mean “no market controls,” you mean “fewer than I’d like.” My insurance company negotiates drug discounts with pharmaceutical companies, engages in risk-sharing, requires me to cost-share, provides me with price incentives to take mail-order prescriptions, and requires me to order my medications off of a formulary. All this, without government mandates. And that’s just on the pharmaceutical side.
I don’t think this is a fair argument to make. No one argues that the US health care system isn’t wasteful. In fact, no one also argues that the European health care systems aren’t wasteful. There is a lot of waste going on in the health care business. The existence of waste doesn’t demonstrate the need for European health care.
One thing your argument does not cover is the way socialized medicine changes the incentives to doctors. In the private health-care market, doctors may be incented to order too many tests and prescribe too many drugs. In a European-style socialized system, doctors are incented to order too few tests and prescribe only those medications that meet government-mandated “cost effectiveness” guidelines. If a patient’s condition happens to be atypical, doctors will strongly pressure the patient to follow a more “standard” diagnostic and prognostic path, even when that path is inappropriate for the patient. I know because it happened to me.
To a Sumner-style utilitarian, this may seem like an evil you’re prepared to live with. After all, if I want to seek a different path, I can just go to the private sector, right? This argument leaves out two important considerations: (1) This disproportionately affects the poor in a way that offends most people’s sense of social justice, and (2) when the largest provider of health care in a country is the government, the government’s policies and procedures distort the private market, too, making it harder and harder for patients to end up with any sort of health care other than what the government mandates through its cost-controlled public system.
To be fair, I think a two-tiered system is preferable to a single-payer system. But it’s worse than the existing US health care system on criteria that matter to me.
Hazel Meade
Nov 1 2018 at 12:58pm
The reasons why what American progressives want, i.e. “single payer” is NOT what European style health care is like, is worth quite a few blog posts on it’s own.
The thing is that when most people talk about “single payer” what they imagine is a free, government-run health service in addition to private health care. i.e. an expanded medicaid or medicare. But what is actually proposed is a system in which only the government pays for health care – thus the “single” in “single payer”. The reason for that is that “single payer” is NOT about providing minimal health care to the needy it is about equalizing health care treatment across the population. If private health care is allowed to exist along side a single payer system, richer patients will pay extra to jump the line and get better treatment. Doctors will drop out of the public system and cause shortages which will make the public system increasingly bad, causing more patients to line jump, and you will end up with a two-tier system, public care for the poor, and private care for anyone who can afford it. But that’s not what progressives want – they want the poor to get just as good treatment as the rich.
Alan Goldhammer
Nov 1 2018 at 2:46pm
Hazel writes,
“If private health care is allowed to exist along side a single payer system, richer patients will pay extra to jump the line and get better treatment. Doctors will drop out of the public system and cause shortages which will make the public system increasingly bad, causing more patients to line jump, and you will end up with a two-tier system, public care for the poor, and private care for anyone who can afford it.”
Doctors are already dropping out of the system. You are seeing some who refuse to take on Medicare patients and others who are forming concierge practices and do not accept any insurance. In our area two major hospitals were taken over by a major university health system in our state and now all doctor who want to practice at those hospitals or have admitting privileges must join the university health system practice. The US system is terribly balkanized compared to almost every other western country’s health system. It’s interesting from the Reid book that I referenced earlier is that Japan has the highest rate of physician visits of the countries he writes about but still manage to contain costs.
Hazel Meade
Nov 1 2018 at 5:18pm
Well, right. Obviously, what we ave now allows rich people to get better health care, and leaves those reliant on the public system worse off. My point is that IF you had a single payer system and didn’t ban private health care, you would end up with a tiered system, like what we have now. The explicit goal of single-payer is to equalize health care treatment, not to have a system where rich people get better health care than poor people.That’s what Scott is arguing – you could have an el-cheapo “free” public system and have a private free market tier that wealthier people layer on top of it. That’s what much of Europe does. My point is That’s not what progressives really want.
Alan Goldhammer
Nov 1 2018 at 5:37pm
Again, I would urge you to read TR Reid’s book. Certainly one can find much to complain about the NHS in the UK which is the truest version of single payer government run health care in Europe. However, it’s not the only model as France, German, Switzerland and The Netherlands have shown. They all have taken different approaches to universal coverage. Universal coverage does not have to be the NHS model. It also can be a private insurance model. Personally, I’m agnostic on the version as I see merits in almost all approaches.
Hazel Meade
Nov 2 2018 at 1:03pm
Right, well, “universal coverage” doesn’t have to mean “single payer”. That just happens to be what progressives are advocating – because they don’t just want universal coverage – they want equal coverage.
Hazel Meade
Nov 1 2018 at 5:26pm
Let me put this a different way.
Imagine in this tiered system that the cheap public system didn’t allow women under 50 to get free mammograms every year. How long to you think it would take before progressives started demanding that the “cheap” public system pay for free mammograms for 40 year old women? What if long waiting lines for mammograms resulted in a shortage of mammogram machines in the public sector? How long do you think it would be before they started complaining that poor people were dying of breast cancers because they couldn’t afford to pay for the private sector mammograms?
Hazel Meade
Nov 1 2018 at 5:34pm
Now generalize this concept to any health care problem:
A poor person suffers from/died from X, which they would have been treated for if they could afford to pay for treatment Y, which is only available(in a reasonable time) to people with money to afford private health care.
There is literally no point on which that argument is any different from any issues with any poor person being unable to afford treatment right now, whether in a hybrid or fully private system.
As long as there is ANY private sector health care, you can’t get rid of the problem that “some people can afford Y, and other people can’t.” The only way you can make sure that nobody dies of something that someone else can pay to be treated for is to eliminate free market health care and make the government ration it out on a random basis.
Jan Haugen
Nov 2 2018 at 1:50pm
Most First World systems DO allow, use or heavily use private health care. I urge you to look at how it works out, because it does not go much like you extrapolate.
Everyone can have a mammogram every year if they want. But most don’t. Getting people to go to the doctor as often as the should and do the test they should are far more of a problem than overutilization. Outside of the parts of the US environment that restricts healthcare heavily by cost to the point where it becomes a desirable item due to its sheer scarcity, people don’t much enjoy going to the doctors and find all sorts of reasons not to.
Scott Sumner
Nov 1 2018 at 1:20pm
Duncan, The lucky country.
RPLong, You said:
“You ought to first establish that the money Americans are voluntarily spending on health care is wasteful.”
That’s easy, the money I and the people I know spend on healthcare is very wasteful. Why assume that we are atypical? Plus, economic theory predicts that private spending will be wasteful when it’s massively subsidized.
I agree that the European system leads to healthcare decisions that hurt health, as does the US system. It’s not clear to me that the US system is better for the poor, as you seem to suggest.
I consider both the European and American system to be “socialized medicine”, and I’m opposed to both systems. I just think the European system is clearly less bad. And it’s not more socialist, at least in terms of government spending as a share of GDP.
Hazel, OK, but if you ask them if they’d like the Swiss system, don’t they say “yes”? I’ve seen articles where progressives praise the Swiss system.
Hazel Meade
Nov 1 2018 at 1:42pm
Are you sure that progressives have any idea what the Swiss system actually is? Most progressives I have met seem to assume that all health care in Europe is government run.
Incidentally, the Swiss system is basically the ACA, isn’t it?
Ahmed Fares
Nov 1 2018 at 1:45pm
A point on how Canadian single-payer differs from government funded healthcare.
In single-payer, while the government foots the bill, there is still competition. Doctors still have to compete with each other for patients so the incentive is still there, i.e., you still retain the benefit of a market system.
Another point to mention is “defensive medicine”. The US is a litigious society. Doctors order a lot of unnecessary tests to avoid being sued and having their malpractice insurance rates rise. Besides raising the cost of healthcare, these unnecessary tests also increase patient risk. Think hospital-acquired infections here or the complications from unnecessary surgery. This is even before you get to the problems inherent in for-profit medicine.
In Canada, doctors follow certain mandated protocols. As long as they follow these protocols, they can’t be sued. This goes a long way in reducing costs.
Scott Sumner
Nov 1 2018 at 4:56pm
I agree about defensive medicine. But keep in mind that the Canadian system does not differ from government funded healthcare, it is government funded healthcare.
Hazel Meade
Nov 1 2018 at 5:13pm
I disagree.
In Canada, prices are fixed by the government, so the patient has little basis to comparison shop. Doctors that are “good” will just be booked up the fastest and have the longest lines. But they can’t really make more money, so there is no incentive to be “the best”.
The mandated protocols limit competition and innovation. Everyone follows a standard procedure. And who decides what the mandated protocol is and whether to prioritize cost or efficacy?
Parleo
Nov 2 2018 at 6:38am
I have lived in 2 EU countries and one benefit that I feel is very important is the time and energy saved researching & buying insurance, and then dealing with them when it comes time to actually use it. The best thing for me about typical EU style healthcare is that, unless I am ill, I never ever think about it.
Brian Donohue
Nov 2 2018 at 1:12pm
8% of GDP- damn, that’s $5,200 per capita. Seems like reasonable wherewithal to provide basic + catastrophic coverage. We’re already doing socialized medicine, just incredibly inefficiently.
Jan Haugen
Nov 2 2018 at 1:16pm
Scott, I don’t disagree with you. At all. There are a few things I’d like to add though.
As far as I know a lot, if not most, of the extra costs of the US system originate in the plethora of systems, providers and payments, and their trying to interact. That generates a vast bureaucracy. I’ve seen a study showing that just the processing of payments cost almost 500 billion per year. 500 billion is nearly 1/6th of the total US healthcare spending, and more than the yearly military budget of the US.
It almost doesn’t matter which specific UHC model the US adopts. Insurance-based Bismarck style like Germany, Switzerland etc, the NHS style Beveridge type of the UK and Scandinavia, or the national insurance model of Canada, Taiwan etc. They are different from each other and from our European perspective the differences seem significant, but the US spending and results are so far out of whack with the rest of us that it almost doesn’t matter which one you pick. Just pick a system, implement it and let private provision fill in any gaps. Its what most of the rest of the world do.
You are far past the point where crafting a bespoke system should be a priority.
Which is what you are saying I guess.
There is no “European system” Some European nations use NHS type systems with their own varieties. Some use for-profit insurance, some use hybrid setups. The US is special in trying to use all of them. Often with the feedback controls taken off. The UK, Scandinavia and Iberia uses varieties of what is known as Beveridge style systems. The US VHA system is a similar setup but without the media interest that are quick to lash mistakes in those nations. Medicare is a National Insurance model. Employer-provided healthcare pools is Bismarck like Germany, the Nederlands and Switzerland. Out of pocket for the uninsured is the way they do it in the rural third world.
On cancer, the incidence increases sharply with age. And it is one of the top killers today. Most comparisons do not correct for the US shorter lifespans. A number of the people who get diagnosed in Europe are already past the average lifespan of the US. That makes US stats look better.
I am not that impressed with the Singapore system. It seems heavily coercive to me. There is no evidence that I know of that the population of nations affect healthcare cost much, but population density though, can have a significant effect on costs. And if you can cover your entire population from a single hospital, you can save a lot of money. Compare Singapore to other city-states and their costs are not that far out of line.
Jan Haugen
Nov 2 2018 at 2:08pm
I live outside the US. Let me try to describe how I see US healthcare with an analogy: We provide healthcare like K-12 education. We’ve basically decided for both that its fairer and better for the nation if everyone has a right to that. We build some hospitals like we do schools. Buy some equipment, labs and computers for the schools, labs and MRIs etc for the hospitals. Hire some teachers for the schools. Doctors, nurse etc for the health care.
People move to an area, they register with a doctor. They register their kids with the school district. I mean you can do both private if you want, but it’d be expensive and not gain you much if anything.
Consider if you provided K-12 education the way you provide healthcare. Have to get insurance. No pre-existing pregnancies or kids. If you didn’t have insurance your kid doesn’t get any education. Except if you pay through the nose privately. Insurance does not necessarily cover all classes. Might not cover maths, or history or something else. Some schools are in your network, some are not. A large number of education insurance companies out there. Six hundred thousand people working for them and making good money. Schools have more people dealing with payment paperwork and liaising with insurance than they have teachers. Its a massive expense to people and results are poor. A few groups are exempt, about 33% of the population. They get government schools. Half a trillion dollars spent on processing payments.
Does that sound mad? Its what your healthcare system looks like from the outside.
(To get the analogy you have to overlook the possibility of home schooling. It breaks down a bit there. You can home school a kid but you can’t do home brain surgery)
robc
Nov 2 2018 at 5:26pm
And yet, if you cut off your hand, you still want to fly to Kleinart-Kutz in Louisville, KY, USA, no matter where in the world you are.
And a majority of their doctors went to medical school outside the US. Weird that they would come here with the crappy system in place.
Or maybe the system, as crappy as it is, still provides the best incentives in certain cases.
Jan Haugen
Nov 5 2018 at 7:42am
Why on earth would you try to fly to the US from elsewhere in the world with an amputated hand? It seems that quick action with reattaching nerves and blood vessels before tissue death might be top of your priorities.
Besides that…why would anyone go to the US for treatment ? Its not like people from around the world carry US insurance , so it’d be out of pocket. Which means not only massively greater but also more unpredictable costs. And that is before getting into the quality issues. The US does poorly in terms of hospital errors, amenable mortality.
The way markets work, it should not be surprising there is a massive flood of patients leaving the US for treatment, entirely dwarfing the number that enter. Its one of the greatest rejections of a system by citizens voting with their feet since East Germany.
About 100 000 people come to the US for medical treatment per year. Cosmetic surgery, rich people from third-world nations etc. Meanwhile between 1,5 – 2 million people leave the US for medical treatment each year. In 2002 Katz et al surveyed the US hospitals within 100 miles of the border and found that about 600 Canadians crossed the border for healthcare each year.
Just Ontario in Canada estimated 600 000 cases of Americans getting free healthcare on fraudulent documentation per year. (Granted, this is not as hard a number, since this is a crime, surveying it is more difficult. And the number is older)
This is how markets work. American healthcare is far more expensive, cost is less predictable and rates of medical and lab errors higher. It should not surprise anyone that the people who have the opportunity elect treatment elsewhere. Although large sections of health care have very little price elasticity so there is a big segment of the market that acts as a captive market.
robc
Nov 5 2018 at 8:48am
And yet, people do. While it was 25-30 years ago, I know this was done for the son of a professor of mine. When I told him I was from Louisville, he told me the story. His son cut off 3 fingers in a Kibbutz in Israel. And they were reattached in Louisville. He lost one of them, but that was due to a delay caused by the Israeli government.
Jan Haugen
Nov 9 2018 at 6:39am
Well, I am not going to say that is impossible, but it seems exceedingly strange. Today, digits can be replanted after very long delays if kept well. 30 years ago? Not so sure. Generally, less than 12 hours if warm for a finger or 24 if cold. Today. It is generally stated that irreversible ischemic injury occurs after 2–4 hours of warm ischemia and 6–8 hours of cold ischemia time.
Flight time from Tel Aviv to Miami is over 13 hours. Today. With no waits, booking times etc, just the straight flying time.
Replanting a digit isn’t that much of a thing today. It was sensational fifty years ago when those two Japanese did the first one. But I have some difficulty believing that developed nations were not doing that frequently in the early 90s. And it seems Israel would have more experience than most with trauma surgery.
So not impossible, but it sounds like there were very special circumstances involved, or some very questionable medical calls were made.
It appears likely that he’d have kept all his fingers if he had gotten the surgery right away in Israel or Europe.
Also, health care costs in the 88-98 period were not as divergent as they are today. US healthcare costs started accelerating faster than the rest of the world in 1980.
Thaomas
Nov 2 2018 at 7:35pm
Your plan, provided it included the amount that the government spends on subsidies to employees and employers for health care insurance, was financed by a VAT or progressive consumption tax instead of a wage tax, and be used to purchase medical services abroad could have been the GOP’s “replace” of their ACA “repeal and replace” plan. I’ll bet a lot of Democrats would have supported it and the ones who did not would have a hard time making health insurance an issue.
michael pettengill
Nov 3 2018 at 3:25am
I agree as a liberal. Adopting the German system which is similar to McCain’s 2008 plan would be efficient, very fair, and provide better cash to 98% of the population.
I’d prefer the Israeli system of HMOs which put doctors in charge of balancing prevention, risk, cure, based on my decade plus with a great NH HMO before the 80s tax reform forced HMOs to split risk from delivery to impute profits to the insurer to be taxed like for profit insurers were taxed on profits, “to level the playing field”.
But you do understand that killing say 1% of total jobs/incomes per year as the system is phased in will cut GDP for 5-8 years.
Such cuts will hit blue States, Texas, Florida economies hard, but not West Virginia, Kentucky, etc much.
Of course, the GOP in Congress will block it because members will object to their pay as medical professionals being slashed by over half to 90%.
Benjamin Cole
Nov 3 2018 at 11:14am
The Fable of Singapore will never die.
I like small government too.
But in healthcare in Singapore, as in every other aspect of the Singapore economy, the government is pervasive and directing.
“Since the 1990s, all public hospitals, polyclinics, and specialty centres [in Singapore] have been restructured as government-owned corporations, and operate under three healthcare groups or “clusters”:
National Healthcare Group
National University Health System
SingHealth”
Wikipedia.
Imagine the US, in which all the hospitals were owned by Uncle Sam. They have universal health care in Singapore, and some public-private mixing too.
But maybe the Singaporeans are onto something.
The US federal government run a huge healthcare system, for former federal employees. Federal hospitals—172 of them— staffed by federal employee doctors, nurses, administrators, an so on. Many more clinics, etc. It’s called the VA, and open to 20 million veterans, free of charge.
No one suggests privatizing the VA, so I guess it works okay.
In addition, everyone seems happy with the military hospitals, such as Walter Reed National Military Medical Center.
Government-owned hospitals and universal healthcare seems to work in Singapore, and in the US military and veterans services.
Scott Sumner
Nov 3 2018 at 11:24am
Parleo, I also hate our insurance system, way too much paperwork. I’d prefer to pay out of pocket, and not through insurance.
Jan, I am aware that there are a variety of Europeans systems, my point is that the governments tends to spend around 8% of GDP and cover almost the entire population. I don’t find your comments on Singapore to be at all persuasive. Their government spends only 2% of GDP, and their outcomes are just as good as in Europe. The fact that Singapore is urban is not a big factor; most European countries are 80% urban, so that doesn’t explain the 4 to 1 (public) cost discrepancy. Europeans need to face the fact that Singapore has a much better economic regime than they do, which is why places like Italy are struggling so much. Europe needs to reform its economy, especially in the south. (The US also needs reform.)
Thaomas, I assure you that Democrats (and the GOP) would strongly oppose my proposal.
Jan Haugen
Nov 9 2018 at 7:50am
2% ? Thats a bit low, isn’t it? Or have they cut their spending massively lately? The latest comparison years I am aware of is 2015, and they passed 4 % there with 5 % projected for 2020. For comparison, Monaco spent 4,3 %, San Marino 6,1 %, and Andorra 8,1 %. (2014) Which works out to a fairly similar amount in PPP dollars.
Population density is not the only factor that matters for spending of course. But its not just urban versus rural, but many centers versus one.
Seppo Mäntylä
Nov 4 2018 at 7:56am
Living currently in my fourth European country and frequenting fifth (my wife’s home country), I see plenty of bad things in European healthcare systems as well.
There are huge hidden costs caused by the necessity of gatekeepers that are required to do perform this “prioritisation”. Usually end result is something like this:
Instead of visiting an ear doctor because you have ear pain, you actually have a consultancy with a nurse. She prescribes you with ibuprofen and sends you home with the instructions to come again if things don’t get better in 48 hours.
In two days you come to meet a GP, who looks at your ear, says: “uhmm”, prescribes you something and sends you home. Then you come again when it still doesn’t help. On the third visit you get referred to ear specialist who finds the cure in 5 minutes and the whole process took some 3 weeks of discomfort.
Because all of this is “free” and you pay 45% tax-rate, you don’t really feel like paying private doctor if you can somehow avoid it, because with your 2500eur take home salary paying 200eur for specialist visit doesn’t seem like a nice idea when you have a family to support.
Insurance based systems have the incentive issues that you already mention.
As flawed as the American system currently is, I think the real solutions are to be found from supply side reforms, not by copying the European gatekeeper model that is very customer unfriendly. This is not to say that European models are horrible, it is just that better options are out there. Reality is that if you let healthcare professionals do the prioritisation, they will come up with somewhat functional system, but the friction created by this gatekeeper system is still there.
Just fix (axe) healthcare supply side regulation and things will get considerably better. Most likely you don’t even need to do anything for demand side. If you manage to lower the costs by deregulating, then more people can afford to pay from their own pockets and insurance schemes will pop up for more cost conscious customers.
Seppo Mäntylä
Nov 4 2018 at 9:04am
Addendum: European systems are very diverse as stated by others. The example above is more like UK NHS style service.
Insurance based systems of Germany and Switzerland are somewhat different. Though I remember distinctively when my wife needed to go to gynaecologist in Germany and multiple clinics said that they don’t take new patients with public (almost 700€/month) insurance. Because of this one occurrence, I dislike the German and due to other horrible experiences the UK system.
Swiss one seems the best, from customer perspective, though since it is an insurance based systems they have a problems with the costs slowly creeping upwards.
Jan Haugen
Nov 5 2018 at 7:46am
The Swiss system tends to score very high for responsiveness, efficiency and lack of waits. It does however tend to be one of the most expensive systems out there, often clocking in a 2/3rds of US costs.
Mark Bahner
Nov 5 2018 at 10:48am
While we’re recommending things that are never going to happen for political reasons, I’ll also note that a significant proportion of total Medicare spending comes in the last year of life. (In fact, it’s 25% of Medicare spending on people older than 65 that comes in the last year of life, per Juliette Cubanski, et al.) So I say, “‘Death panels?’ Bring ’em on!”
By that I mean that there should be some consideration for how long a person has already lived and can expect to live, in the rationing of government health care spending.
Jan Haugen
Nov 9 2018 at 6:42am
It is often difficult to know in advance which year of life is going to be the last one. Not always but often. I mean, if you were to withdraw medical care that would help make sure in many cases, but I don’t think its a good way to go.
Nick
Nov 9 2018 at 12:51am
What leaves me stumped about health care is that it is unnecessarily politicised. Imagine a world where laptops are unnecessarily expensive and a politician comes up with an “electronics for all” campaign proposing ridiculous regulation and taxation on electronic device manufacturers. Wouldn’t you be able to see through this BS instantly?
It’s the same with healthcare. Why would you not let the private industry operate unscathed, especially after we know how government operated industries perform? Why, why would anyone politicise a peaceful activity and deviate from the libertarian recommendation, if for no other purpose than political entrepreneurship? The free market provides other stuff, what’s so difficult about healthcare?
If progressives really liked improving people’s healthcare, they would be able to do it now. Why wait until the next election to simply setup a private company that is altruistic in its motivations, relies on a market process (for instance, set up as a profitable business) to provide all the supposed benefits from their “single payer” system?
This is essentially the common sense argument for libertarianism. Would you politicise other peaceful activities that you do everyday? Would you take to the streets protesting every time you felt hungry or wanted to brush your teeth or learn quantum computing? I’m guessing not.
I’m not denying that there exist perverse incentives in the healthcare industry, but before you institute a massive body of government to “cancel” those incentives, you need to demonstrate, beyond any doubt, that organisations like FDA do not hurt/kill people through unintended consequences (which is not true, people die every year because they are denied treatment because of the FDA) and there cannot be free market solutions (like setting up a private company with altruistic motivations).
Comments are closed.