In 2010, there was an growing problem of people abusing painkillers such as OxyContin. Unfortunately, the steps taken to address the crisis may have made things even worse. A 2018 NBER study by William N. Evans, Ethan Lieber, and Patrick Power showed that when the pills were reformulated to reduce drug abuse, people switched to other drugs such as heroin, which were even more dangerous:
We attribute the recent quadrupling of heroin death rates to the August, 2010 reformulation of an oft-abused prescription opioid, OxyContin. The new abuse-deterrent formulation led many consumers to substitute to an inexpensive alternative, heroin. Using structural break techniques and variation in substitution risk, we find that opioid consumption stops rising in August, 2010, heroin deaths begin climbing the following month, and growth in heroin deaths was greater in areas with greater pre-reformulation access to heroin and opioids. The reformulation did not generate a reduction in combined heroin and opioid mortality—each prevented opioid death was replaced with a heroin death.
In addition, the government has begun pressuring doctors not to prescribe opioid painkillers.
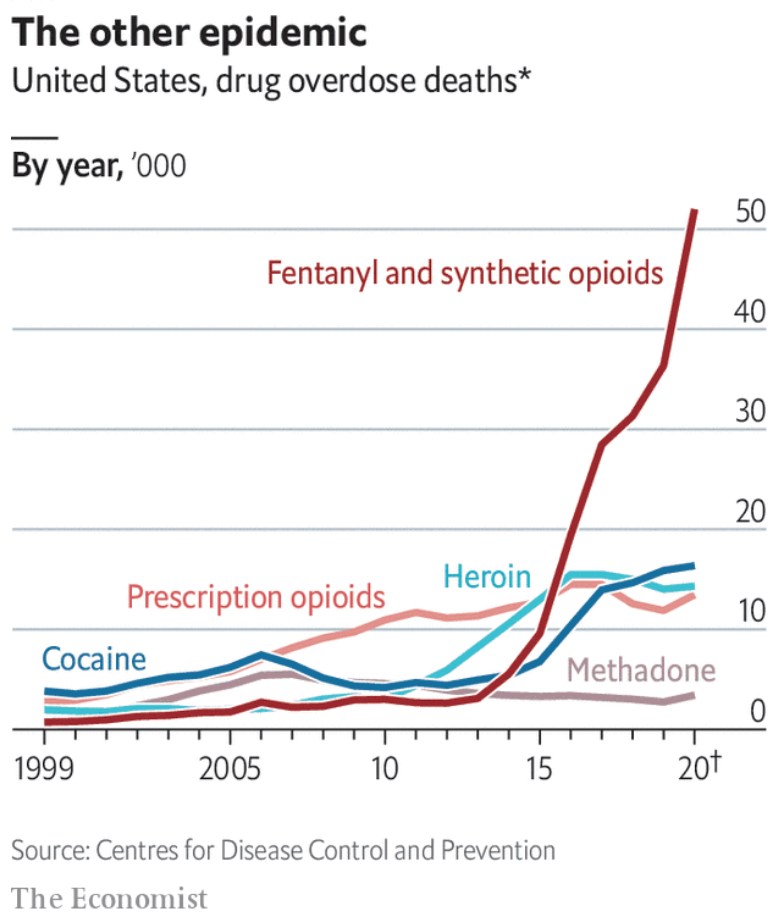
The Economist has a graph showing that since this study, thing have gotten even worse:
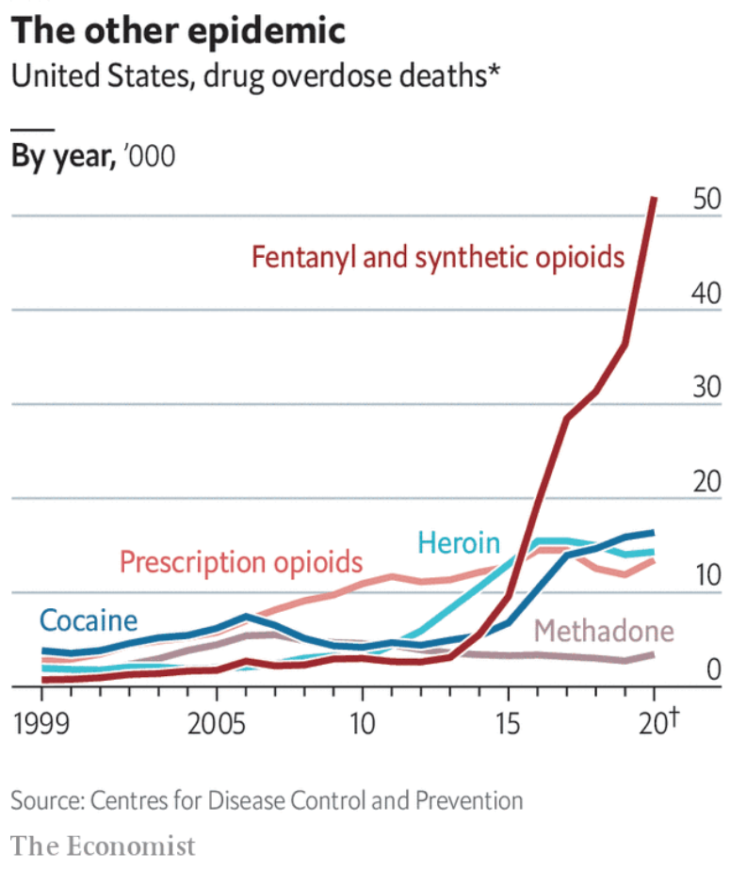
Notice that fentanyl deaths are now far higher than before the government began cracking down on painkiller use. That’s because fentanyl is far more dangerous:
The drug’s potency makes it easy to misjudge dosage, especially for new users without a tolerance. Increasingly, counterfeit prescription pills, resembling oxycodone tablets or benzodiazepines such as Xanax, contain fentanyl. Brad Finegood, an adviser to the public-health department for Seattle and King County, says he has seen lots of unsuspecting people casually take a fentanyl-laced pill and die.
It sounds “responsible” to crack down on the abuse of addictive painkillers, but the unintended side effects may well be even worse than the original problem. Politico has an excellent piece on the effects of cutting off pain medication to those with severe chronic pain:
Last August, Jon Fowlkes told his wife he planned to kill himself.
The former law enforcement officer was in constant pain after his doctor had abruptly cut off the twice-a-day OxyContin that had helped him endure excruciating back pain from a motorcycle crash almost two decades ago that had left him nearly paralyzed despite multiple surgeries.
“I came into the office one day and he said, ‘You have to find another doctor. You can’t come here anymore,’” Fowlkes, 58, recalled. The doctor gave him one last prescription and sent him away.
Like many Americans with chronic, disabling pain, Fowlkes felt angry and betrayed as state and federal regulators, starting in the Obama years and intensifying under President Donald Trump, cracked down on opioid prescribing to reduce the toll of overdose deaths. Hundreds of patients responding to a POLITICO reader survey told similar stories of being suddenly refused prescriptions for medications they’d relied on for years — sometimes just to get out of bed in the morning — and left to suffer untreated pain on top of withdrawal symptoms like vomiting and insomnia.
More recently, the Washington Post has an article with lots of similar stories:
Hank, 79, has had seven shoulder surgeries, lung cancer, open-heart surgery, a blown-out knee and lifelong complications from a clubfoot. He has a fentanyl patch on his belly to treat his chronic shoulder pain. He replaces the patch every three days, supplementing the slow-release fentanyl with pills containing hydrocodone.
But to the Skinners’ dismay, Hank is now going through what is known as a forced taper. That’s when a chronic pain patient has to switch to a lower dosage of medication. His doctor, Hank says, has cut his fentanyl dosage by 50 percent — and Hank’s not happy about it. He already struggles to sleep through the night, as Carol can attest.
“He’s moaning, he’s groaning, he’s yelling out in pain,” Carol says.
“Why am I being singled out? I took it as prescribed. I didn’t abuse it,” Hank says.
He is part of a sweeping change in chronic pain management — the tapering of millions of patients who have been relying, in many case for years, on high doses of opioids.
I’m not even in favor of treating a 29-year old this way, although I can sort of follow the logic. But let’s face it, a 79-year old who’s had lung cancer and heart disease is on his last legs. Why can’t he live out his brief time remaining without being tortured by pain?
The argument for drug regulation is that people might abuse drugs if they weren’t required to get a prescription from a doctor. I don’t believe that the benefits of drug regulation outweigh the costs, but it’s at least a plausible argument. But now we are saying that we don’t even trust doctors to act in the best interest of their patients. Instead, we seem to believe that DEA agents who have never met the patient should make the decision. Here’s Politico:
“I will no longer treat chronic pain. Period,” said Sue Lewis, a primary care doctor who works in an urgent care clinic in Portland, Oregon. “There is too much risk involved,” she said, adding that if a patient doesn’t take the medications as she prescribes them, they could jeopardize her license.
Steven Henson, an emergency room doctor in Wichita, Kansas, described how his license was suspended after six patients illegally sold the medications he prescribed, without his knowledge.
“The DEA should be working with doctors when this happens,” as opposed to punishing them, Henson said.
There will never be a perfect solution to the problem of addictive drugs (including alcohol.) We should be focusing on minimizing the damage. In most cases, the least bad outcomes will occur when the decision making process is decentralized, with those closest to the issue making their choices. When it comes to federal regulation, we should never lose sight of the Hippocratic oath: First, do no harm. When I look at the soaring rate of fentanyl deaths, I suspect that our regulatory regime hasn’t even met that minimal threshold, and that’s not even counting the cost of pain that is no longer being managed.
PS. I wonder if the attempt to demonize drugmakers has contributed to our policy overreaction. The same issue of The Economist has a review of a new book that critiques the role of the Sackler family, which controls the drugmaker that introduced and promoted OxyContin:
Shiftless third-generation types are rendered with evident loathing, skilfully skewered by their own words in court or by Mr Keefe’s (anonymous) sources. One aspiring fashionista wishes an obstreperous journalist would focus less on her last name and more on the hoodies she designs.
Really? Is it unreasonable to want people to judge you on your career and not on your last name? During the Chinese Cultural Revolution, people were punished because their parents had been capitalists. I thought we were beyond that sort of guilt by association.
READER COMMENTS
Mark Z
Jun 3 2021 at 12:08am
Fentanyl has gotten a lot easier to manufacture and can be trafficked much more easily than ‘old-fashioned’ drugs like heroin, since it’s so much more potent and thus takes up less space, so the DEA is even less effective than stopping the flow of illicit opioids. I imagine that makes policymakers feel that the only thing they can do is go after the licit opioid market, and they have to do something (supposedly).
Hopefully though someday after qualified immunity is dispensed with some FDA and DEA higher ups will be subject to a class action law suit by all the pain patients they’ve needlessly tortured over the years and be bankrupted like the Sacklers. (joking of course, I’m sure it’s not legally viable, but they do probably deserve it).
Philo
Jun 3 2021 at 10:49am
Bad laws, such as the drug laws, promote contempt for the law. Given his circumstances, Hank rightly rejects, at least as it applies to him, the law that would deprive him of the drug(s) he needs to alleviate pain. Before attempting suicide, he should seek out an illegal supplier.
Michael Sandifer
Jun 3 2021 at 12:20pm
Yes, a combination of changes in regulation and Medicare rules regarding Suboxone coverage contributed to my mother’s overdose death. The change in regulation forced her to change doctors, though the one she was seeing was the only one who ever developed a medication regime that stabilized her drug intake, and Suboxone became unaffordable for her after Medicare stopped covering it. She only lasted about a year without Suboxone.
Scott Sumner
Jun 3 2021 at 1:49pm
I’m very sorry to hear that. I don’t think that regulators understand the damage they are doing.
Michael Sandifer
Jun 4 2021 at 1:16am
Thanks, but as Larry David would say, this happened a few years ago, so the sorry window is closed.
Michael Sandifer
Jun 3 2021 at 12:26pm
For those unaware, Suboxone contains both an opioid that is an excellent pain reliever that satisfies opioid cravings, and another agent that helps prevent opioid overdose. Why regulators and Medicare wanted to limit access to that drug, but not the milder opioids that my mother overdosed on, I don’t understand.
bill
Jun 3 2021 at 2:00pm
Every interaction my family has had with a hospital has included a battle to get reasonable pain reduction medication.
Scott Sumner
Jun 3 2021 at 6:22pm
I’ve also seen those situations firsthand. I’m amazed at how callous hospital employees can be when it’s not their own pain involved.
David Lundeen
Jun 6 2021 at 9:39am
I should expect nothing less than total subservience to private power from George Mason University. Mr. Sumner ‘forgot’ to include a brief summary on the history of morphine derived drugs, the difficulty in treating pain for many physicians and how the over-prescription of opioids led to normal people buying black tar heroin. I’ll provide three quick points so this important issue can be properly discussed, and not used as a stick to beat the people.
1) Opium / heroin had always been a fringe drug in the US with few users in select geographies. Huge swaths of people did not suddenly become heroin users overnight. They started on Oxycontin and then later bought black-tar heroin as it’s virtually the same drug.
2) Treatment / Management of pain continues to be an Achilles heal in Medical Programs. There are very limited pathways to treat this. Based on one obscure paper which noted that opiate derived medicine was not addictive, opioids became the only tool for overworked physicians who had too many clients to treat and not enough time (the wonders of the free-market and efficiency).
At it’s peak, Purdue Pharma had over 100,000 Sales Reps. Hospitals and clinics were flooded with these pills, and physicians were only too happy to prescribe these instead of actually spending time with patients to deal with chronic pain.
If we could only consider the entire picture, instead of fantasies promulgated by Mr. Sumner we could develop simple, effective ways to treat this scourge. Instead, this is used as an example to further demonize democracy for it’s one fatal flaw – through public pressure societal changes can be made (David Hume wrote about this too which I suggest reading, along with Adam Smith). Mr. Sumner would rather this not happen so he can continue his cushy position absolving the privileged class for the most egregious of crimes while writing about liberty. Nothing less can be expected from the heirs of George Buchanan and their grotesque disregard for democracy in pursuit of their mathematical religion – economics (which is not a science to be clear).
Tom West
Jun 6 2021 at 10:38pm
Except we have this:
Given that we prohibit non-opiate painkillers that have fatal side effects that are an order of magnitude lower, the real question is how to did these painkillers ever get approved in the first place?
I suspect the state is attempting to correct what they perceive as their initial misstep.
As for Sackler descendants getting bad publicity, there’s a fair number of people (and reporters) who feel the Sacklers are deliberately complicit in what they see as the murder of tens of thousands of Americans. Unfortunate though it might be, those who are living off the proceeds of those “murders” are going to be considered fair game for at least embarrassment by them.
I don’t necessarily agree, but I see the occasional article about the descendants of dictators that escaped their country with a good Swiss bank account, and they’re treated much the same way.
GregS
Jun 8 2021 at 2:45pm
Good post, I just want to clarify one thing.
“In 2010, there was an growing problem of people abusing painkillers such as OxyContin.”
A lot of people think that there was a growing population of opioid addicts in the past two decades, and that simply isn’t true. The statement is technically true if “growing problem” refers to the increase in overdose deaths, but not if it is meant to imply a growing population of addicts. According to statistics gathered by SAMHSA, the number of people who abused prescription pain relievers was flat from 2002 through the present. They actually ask the question in two different ways on their survey. It asks about prescription opioid misuse within the past month, and it (separately) asks if you’ve had an opioid use disorder within the past year. The former should catch casual use, the latter should catch more severe cases of addiction. Both are flat. Bizarrely, they stopped publishing the trendline for this particular category of drugs in their 2015 report, but here’s the 2014 report that shows the trendline:
https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf
(If you pull the numbers year by year and plot them yourself, which I have done, it still looks flat and actually starts declining in more recent years.)
There has certainly been an increase in deaths over the relevant period, and there was an increase in the total tonnage of opioids prescribed. But the narrative that loose prescribing habits created a new class of addicts is just false. (The 8 to 12 percent Tom West cites is an overestimate. There are plenty of studies that yield a much smaller number. It depends on how you filter the data: for people with/without past substance abuse problems, intensity/duration of prescription, etc. The much-derided 1980 Porter and Jick letter actually holds up pretty well.)
See Jeff Miron’s paper Overdosing on Regulation, which I had a hand in writing and editing. We briefly discuss the literature on “risk of addiction.”
https://www.cato.org/policy-analysis/overdosing-regulation-how-government-caused-opioid-epidemic
Comments are closed.