Avik Roy has a highly informative article in Forbes, discussing the pros and cons of the recent House health care bill (which is now before the Senate). He suggests that the proposal offers a number of improvements over the current regime (Obamacare), but also some flaws. One problem is the tax credits:
Unfortunately, the A-plus on the regulatory side is balanced out by a C-minus on the tax credit side. House Speaker Paul Ryan adamantly opposed a means-tested approach to providing financial assistance for premiums, instead insisting on a flat tax credit that remains the same if you’re at the poverty line or nearing six figures.
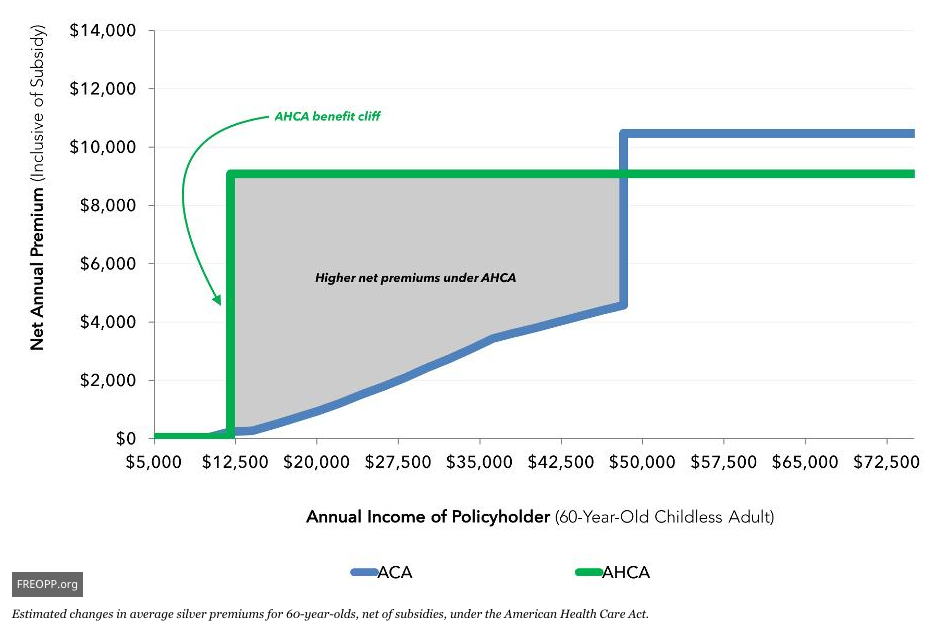
That approach means that millions of low-income Americans in their fifties and sixties will be priced out of the insurance market, while millions of upper-income Americans who don’t need the help will get a big tax credit. Many of the people adversely affected by the AHCA are Trump voters whose favored candidate campaigned on “insurance for everybody.”
Furthermore, the Ryancare tax credit will trap millions in poverty, by slapping them with thousands of dollars in health insurance premiums should they make enough to no longer be eligible for Medicaid. That will discourage the poor from working and rejoining the economy.
On top of all that, Ryancare does nothing to reform the unlimited tax break for employer-based coverage that does so much to make insurance unaffordable for everyone. Indeed, the bill takes Obamacare’s “Cadillac Tax,” an imperfect reform in the right direction, and pushes it back to 2023.
He then discusses some problems with the Medicaid reforms. Roy then concludes with a discussion of how the Senate might improve the bill:
A working group of a dozen GOP senators, derived from the key Senate health care committees–Finance; Health, Education, Labor, and Pensions; and Budget–has been meeting for weeks to contemplate how the Senate should proceed.
That could be a good thing or a bad thing. The best-case scenario is that the Senate builds on the House’s Medicaid reforms while replacing the Ryancare tax credits with a more means-tested version.
One worst-case scenario is that the Senate simply waters down the reforms in the House bill for a result much closer to the status quo.
Another worst-case scenario would be for the Senate to pass the House bill as is. That bill, if it were enacted into law, would price millions of lower-income Americans out of their coverage.
Not only would that policy result threaten GOP majorities in Congress and across the country, it would damage the credibility of free-market health reforms for a generation.
We’ll know soon enough which path the Senate has chosen.
I’ll watch these issues closely as the Senate starts to deliberate on this issue. I’m generally an optimist, but not when it comes to Congress doing the right thing.
PS. For me, the delay in the Cadillac tax was the deal breaker, which showed that the House GOP was not willing to challenge the medical industrial complex that has wrapped its tentacles around 18% of our GDP.
READER COMMENTS
AlanG
May 13 2017 at 11:47am
I’ve been following healthcare reform both professionally and also in retirement ever since Paul Elwood convened the Jackson Hole discussion group almost 30 years ago. For a lot of reasons the current system is irretrievably broken and Obamacare (which I supported) was merely a kludge to try to repair the part that disadvantaged who do not have employer paid for insurance (my two daughters at various parts of their career had/have Obamacare policies but did not qualify for any subsidy).
Perhaps the two best books to read on the topic are TR Reid’s “The Healing of America: A Global Quest for Cheaper, Better Fairer Healthcare” that was written back in 2009 and a more recent book, Elisabeth Rosenthal’s “An American Sickness: How Healthcare Became Big Business and How you can Take it Back.” Reid’s book is valuable in that he compares the US system with 6-7 foreign systems and specifically what those systems might offer in terms of treating a long term chronic shoulder condition as the result of a military injury. It’s instructive that he gets an appointment with one of the leading orthopedic specialists in Japan within 24 hours; try to do this in the US!
Rosenthal documents how medicine has become corporatized (probably not a word, but you saw it here first). Look at all the hospital mergers that are taking place and the so-called “non-profit” hospitals that are raising fees way in excess of what a true non-profit hospital should. All this takes place in the absence of any anti-trust actions from the government. This shrinks down choice and reduces competition. It also forces MDs to align themselves with the hospital as there is no other choice. We are seeing a big move in my area with Johns Hopkins doing exactly this.
There is probably 40% wastage in the current system that will never be squeezed out in the absence of moving to some form of single payer system. The IT infrastructure is appalling (when I was retiring in 2010 I went to talk with David Blumenthal at HHS about possibly coming over to work on this issue as it was something that I worked on in the pharma industry. It was apparent from that one interview that nobody knew what to do and that things were and still are so fragmented that it would be quite difficult to achieve anything. Right now we have two major vendors of EMRs that are incompatible with each other.).
There’s a lot of other stuff that I could go into from my time working on these issues but I think for those interested, the two books I recommend will be quite instructive. I’ve read almost all of Roy’s writings on the topic and am not convinced that his approach is viable. You cannot cure a rotten system with a series of band-aids.
Scott Sumner
May 13 2017 at 2:37pm
Alan, I think it partly depends on how people see the current system. Those who think we have socialized medicine favor a free market regime. Those who think we have a free market regime favor socialized medicine.
I’m in the group that thinks we currently have socialized medicine, and favor shifting to a free market model. I believe that free market competition could cut the cost of healthcare by 70% or more.
AlanG
May 13 2017 at 5:20pm
Scott, I wish I could share your optimism but I think the free market train is never going to get out of the station. Rosenthal’s book that I cited does provide a series of guidelines for how one can take control of some things but it requires a significant amount of effort. One needs to pay close attention to what docs and services are in plan otherwise you get hit with a huge bill. Shopping around is extremely difficult as it is hard to get prices for a lot of stuff (in contrast, France provides pricing for all fees and services and they are usually posted in the office). I needed a lumbar MRI last April and I called four facilities and none would give me the price (it wasn’t all that relevant as I’m on Medicare and they paid for it). How do you assess quality? As Rosenthal points out in her book a lot of women will go back to the hospital where they gave birth regardless of the quality of care it provides.
In order to have competition, one needs a lot of providers and this is where things get sticky. Lots of practices are consolidating and many of them are part of a hospital system. Contractually, they must refer patients to that hospital system if it’s warranted. Hospitals also have the highest costs for all diagnostic tests and once admitted, one is captive to their system.
We are seeing in our area a lot of boutique practices being set up by primary care MDs. One pays ~ $2000/year and that covers unlimited visits. They try to keep the practice size small so you can get an appointment the same day if needed. However, that’s money out of pocket even if you don’t go to the doctor at all that calendar year.
Medicare is OK in that it covers most stuff but one still needs a secondary policy to cover the co-pays. Medicare, which outside the VA is probably most socialistic, is also not free!! It does the best in terms of controlling cost through out the reimbursement system. Hospitals and MDs are forced for the most part to accept payment because of the large size of the patient pool.
Part A, hospitalization, is free and that is the one driving Medicare to insolvency. Part B (doctor visits) has a monthly premium that is means adjusted and Part D (drug benefit) also has a monthly premium. Both require co-pays and the drug benefit varies from provider to provider in terms of what drugs are covered how much is reimbursed. There’s no free lunch there. My wife and I are paying about $14K this calendar year for just our insurance premiums and will probably have close to $1K in co-pays for drugs and other stuff as needed. I honestly don’t know how most seniors make it through the year if they haven’t saved enough for retirement.
The only private sector approach that ever stood a chance was the Fuchs/Emmanuel healthcare voucher proposal from a decade ago. They proposed a VAT which would provide the money for everyone to buy a private sector insurance policy and do away with Medicaid and Medicare. It made sense to me and I had Zeke come down to PhRMA and give a talk on it.
I think it’s quite telling that Charlie Munger said the US has to go to a single payer system with add on insurance for those who want more benefits following the Berkshire Hathaway annual meeting last weekend. He’s as Republican and pro-market as they come.
The promise of Obamacare was that people could leave their jobs and strike out on their own with some good health insurance options. That’s about to end and it’s too bad.
Michael Byrnes
May 14 2017 at 8:30am
Scott Sumner wrote:
Right now we have a mix of both, and the only politically realistic options in the US are to transition from the current mix of both to a different mix of both.
Scott Sumner
May 14 2017 at 11:15am
Alan, You said:
“I think it’s quite telling that Charlie Munger said the US has to go to a single payer system with add on insurance for those who want more benefits following the Berkshire Hathaway annual meeting last weekend. He’s as Republican and pro-market as they come.”
I think I could find people who are even more pro-market than Munger, so I don’t agree that he’s as pro-market as they come.
On your other points, you are mostly telling me that the current health care market works very poorly. I agree. That’s why I want to totally revamp the system, until it is almost completely unrecognizable. It’s possible that we would still have all those problems, but I doubt it.
AlanG
May 14 2017 at 3:12pm
Scott responds, “On your other points, you are mostly telling me that the current health care market works very poorly. I agree. That’s why I want to totally revamp the system, until it is almost completely unrecognizable. It’s possible that we would still have all those problems, but I doubt it.”
Your approach would work but only with massive government intervention. Hospital systems would have to be broken down into smaller parts. Pricing would have to be totally transparent across the board and anyone that violated this would have to be prosecuted (don’t know any other way to accomplish this). Do you police physician referrals to facilities they might own or have a financial interest in or do you mandate disclosure. There are a lot of other things that would have to be done as well (mandating interoperability of IT systems, including Electronic Medical Records).
Have you written on this at all or are planning to?
Comments are closed.