What’s driving the high price of doctors: market inequality or government entry restrictions? My co-bloggers’ debate reminds me of a random encounter with some striking evidence: The Digest of Education Statistics‘ Table 294.
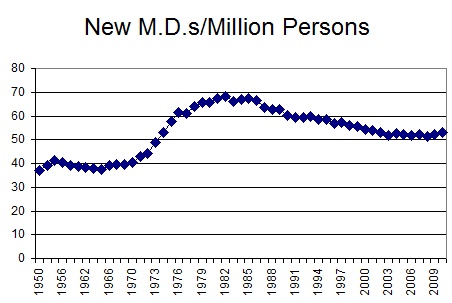
If you peruse this table, you’ll discover that total number of new M.D.s per year has been virtually flat for 30 years. During this period, population increased over 30%. As a result, the new M.D./population ratio has declined for decades.
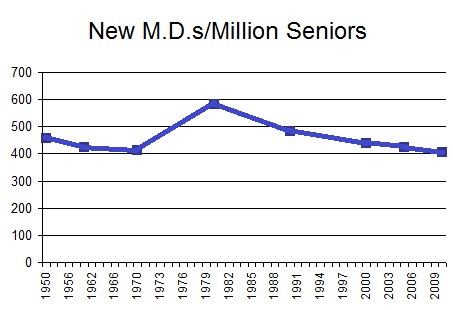
 If you’re not horrified, consider that the senior population – doctors’ best customers – increased by over 50%. As a result, new M.D.s per senior fell by about a third over the last three decades:
If you’re not horrified, consider that the senior population – doctors’ best customers – increased by over 50%. As a result, new M.D.s per senior fell by about a third over the last three decades:
 This is exactly what you’d expect when government imposes rigid numerical quotas in the face of sharply rising demand: a constant quantity regardless of market conditions.
This is exactly what you’d expect when government imposes rigid numerical quotas in the face of sharply rising demand: a constant quantity regardless of market conditions.
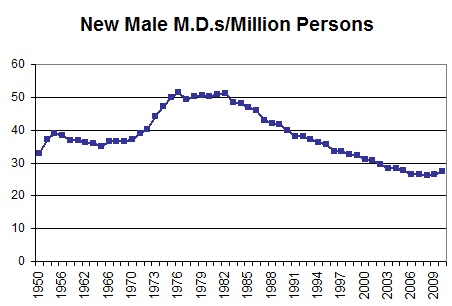
If you’re still not convinced, know this: Over the last thirty years, new female M.D.s have sharply increased. How is this possible given the stagnant total? Because the number of new male M.D.s dropped like a rock! New male M.D.s per person are down by over 45%.
 New male M.D.s per senior are down over 50%:
New male M.D.s per senior are down over 50%:
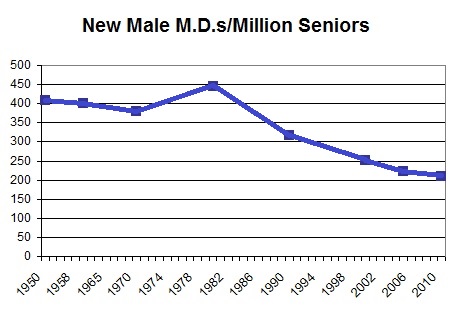 In any normal labor market, massive female entry would have led to a large increase in total workers. But the market for new doctors is anything but normal. The rise in new female doctors has been almost perfectly offset by a matching fall in new male
In any normal labor market, massive female entry would have led to a large increase in total workers. But the market for new doctors is anything but normal. The rise in new female doctors has been almost perfectly offset by a matching fall in new male
doctors.
My point, of course, is not that women have “stolen” men’s places in medical school. My point, rather, is that that draconian government entry barriers are the only credible explanation of the facts. Why else would the number of male doctors have fallen so far relative to demand? Infinitely inelastic demand for medical services? A massive decline in the talent of male applicants to medical school?!
As our population ages, we have naturally seen a large increase in the demand for doctors. If the market for M.D.s worked normally, however, we would have fortuitously experienced a large offsetting supply shock: the rise of the female doctor. Regulation has deprived us of this godsend – and deprived vast numbers of qualified men and women of the right to work in their preferred occupation. Thanks to government entry barriers, demand has gone up and supply is frozen in place. Consumers and taxpayers are paying a fortune for medical care. And the problem is only going to get worse.
READER COMMENTS
gwern
Mar 3 2013 at 9:10pm
Charts don’t seem very impressive: ‘Oh no. We’re back to ratios seen in the 1960s, that well-known hell of skyrocketing extortionate doctor rates.’
Now, one might expect female doctors to work a lot less than male doctors, so we might see a much more dramatic decline in ‘doctor-hours per million people’ and *that* would be very important. But you didn’t provide that.
Peter
Mar 3 2013 at 9:35pm
Why not just let physician’s assistants and nurse practitioners care for people with non life threatening illnesses (sore throat, stuffy nose, etc)to increase the supply of medical providers?
I blogged about some simple changes that would drastically improve medical care in this country
http://pjparlapiano.blogspot.com/2011/07/health-care-problems-solutions-and.html
Fun Fact: More medical schools 100 years ago (166) than today (129)
marc
Mar 3 2013 at 9:37pm
Interesting data. I think if you looked at the number of alternative medical practitioners it would correlate with the decline of scientific practitioners. Alternative medicine is largely based on placebo effects caused by patient-practitioner interactions, and combines a small amount of proven remedies such as diet and exercise with large amounts of what can mostly be considered quackery. The reason people go to alternative medical practitioners is largely because they are plentiful enough that they can spend a significantly longer time interacting with the patients compared to scientific practitioners.
If my hunch is right, strict government regulations such as you describe have essentially increased the attractiveness and use of quackery. How is that for an unintended consequence?
Alan
Mar 3 2013 at 9:46pm
From what I gather, the medical establishment supports this restriction because it increases their own compensation.
I have had a very good doctor tell me that he became a doctor because he thought it was a profession for intelligent people, and was surprised to find that it took relatively little intelligence – just memorization. There are plenty of qualified people, if we will only get rid of unnecessary requirements that are designed to reduce the number of doctors in order to drive up the cost of medical care. The obligatory hazing that keeps many out of the field should also be done away with. Back-to-back 24 hour shifts during residency – what other profession would put up with that, and why would we want sleep-deprived people operating on patients anyway?
jseliger
Mar 3 2013 at 9:49pm
My point, rather, is that that draconian government entry barriers are the only credible explanation of the facts
That’s true, but the market is slowly moving around this blockage through P.A.s and nurse practitioners; I provide links to some discussion of the issue in “Why you should become a nurse or physicians assistant instead of a doctor: the underrated perils of medical school” (which, as the title implies, is mostly about other subject to which the rise of P.A.s and nurse practitioners is also germane).
Brent
Mar 3 2013 at 10:16pm
But Gwern, today those seniors have significantly more demand for medical care (thanks to more wealth, technology, and of course Medicare). Not to mention the rest of the population increasing their demand as well.
Also, it’s not like doctors practice the same way they did in the 1960s. I’m sure there are uncountable ways in which the government, its tort system, and the 3rd party payment system in general have made the typical doctor less productive as far as time spent actually treating patients.
patrick
Mar 3 2013 at 11:18pm
Bryan – is data only available for new MDs? I’m more interested in “active MDs” per [insert unit] of population than just “new MDs.” Hopefully the reason why is fairly intuitive.
Patrick L
Mar 3 2013 at 11:25pm
I saw the first and third graph years ago and looked into it. Doctors are one of the few industries where female entrants reduced male employment.
The choke point is medical school. The total number of potential doctors accepted hasn’t risen with demand, and has possibly shrunk. It very much looks like women who got accepted to medical school were taking spots that would have gone to men.
Medicine is a guild. The guild constrains employment by restraining training. Government regulation doesn’t have to be added to the story to explain it. We may be able to explain in finer fidelity certain specifics, but it’s not necessary. Yes in a free market, capitalistic forces could overcome the guild process by offering substitutes, which in time would erode the market power of the institution, but it’s just one part of the story.
V
Mar 4 2013 at 1:16am
If we agree that total health care system costs (rather than MD salaries**) is the problem facing society, then the evidence that this sort of supply restriction is harming society is negligible.
Given the strong evidence of supply-induced demand in health care (i.e., more doctors in an area means higher health care costs such as in South Florida regardless of health outcomes), poor information transparency, & third party payment skewing incentives, LESS doctors equals lower health care costs and an optimal outcome that is better for society (assuming we don’t magically transform the rest of the system into a free market one).
**MD salaries are only 7-8% of system costs and have been stagnant for 20 years. In addition, if they were too high, the government controls reimbursement rates through the RVU system and can cut them (e.g., ophthalmologists’ and radiologists’ salary cuts in the last 5 years).
Mr. Econotarian
Mar 4 2013 at 3:25am
My understanding is that “Physician and Clinical Services” account for 25% of US health care spending (source), where the definition is:
Tom Amlie
Mar 4 2013 at 10:47am
You just took a HUGE hit to your credibility.
Is this deliberately misleading or is there some reason for your focus on new MDs per million? Isn’t the appropriate measure “physicians per capita”? Looking simply at “new MDs per capita” is worse than useless; it’s almost like you’re viewing MDs as a consumption good; “if the number of new ones each year falls there are fewer MDs”. If we saw that the “new laws passed per million people” fell from one year to the next would you worry that we’re running out of laws? Physicians per capita has more than doubled since 1960. Even that measure is flawed, since there are obvious distinctions between specialists v. generalists.
Tom Amlie
Mar 4 2013 at 10:53am
The number of new physicians annually is not directly relevant, except that it has an impact on the total supply of physicians. The number of physicians per capita has been increasing steadily (dramatically?) since the late 50’s. Does it appear that we’re going to “run out”?
Jeff
Mar 4 2013 at 11:03am
The case is maybe a little overstated because I think the data only shows M.D.’s from US Medical Schools. I gather that the U.S. sucks up a fair amount of healthcare professionals from other countries. Absent immigration, we’d be in even worse shape than we are now.
zdc
Mar 4 2013 at 11:08am
@Peter
The current administration needs you on their side, you’ve got it all figured out. Since you went fishing for views to your blog, I went ahead and replied to your insightful post there.
@Mr. Econotarian
Yes, 25% of CMS expenditures in 2008 went to ‘Physicians and Clinical Servies’. While it looks like you’re trying to refute @V, the numbers your provide at not at odds with the stat stated by @V that physician salaries comprise on the order of 8% of healthcare expenditures. While 25% of CMS expenditures went to physicians, from that money, physicians had to pay office expenses (rent, electricity, office supplies and equipment), staff salaries (nurses, secretaries/schedulers, billing staff/company, accountant) malpractice insurance, licensure and regulatory fees, etc. Of the revenue generate by the physicians services, it wouldn’t be atypical for the physician themselves to be left with 1/3rd or less as pay for themselves. (and the 8% stated by V is about 1/3rd of the 25% you cite).
Ken B
Mar 4 2013 at 12:02pm
When I was an undergrad, my university in Canada had a medical school. The Ontario government decided that rising medical costs were “doctor driven” so reduced the number of places in the medical school. Thus cutting costs and ensuring better health care for Canadians. This is governmental forward thinking at its best!
Ken B
Mar 4 2013 at 1:33pm
gwern
The ambit of medicine is much greater now, and had we sufficient doctors we could treat more conditions successfully. We have in other words more uses for doctors than we had, and not more doctors. So the shortfall can be quite meaningful.
If we had as much computing power per million people as we had in 1982 I think everyone would recognize the opportunity cost.
Ghost of Christmas Past
Mar 4 2013 at 2:37pm
As commenters on an DRH Econlog post just one day ago pointed out, the constraint on new doctors isn’t really medical-school admissions, it is “residency” training slots.
Also, Ken B. brings up an important point, which is that many government decision-makers want to reduce the number of physicians to ration care, not merely because of rent-seeking by the doctors’ cartel. Lots of government types believe that the way to “control healthcare costs” is to restrict the number of physicians so as to limit the amount of care delivered. For the government folks, even if increasing the number of doctors would reduce the prices of the services they perform, that is irrelevant if total utilization might increase because the government people care about (their) overall budget, not individual service prices.
It’s all just another example of how socialized medicine sucks. Individuals would prefer more doctors producing more consumer choice and lower consumer prices. Diverse third-party payers often prefer less consumer choice but generally favor lower consumer prices. But a government medical monopoly prefers less consumer choice and higher consumer prices, for reasons akin to those driving the classical result in economics that a monopolist maximizes profit at a lower level of output, refusing to satisfy demand at prices closer to the marginal cost of production.
C Paxton
Mar 4 2013 at 2:44pm
I think what you’ve provided here is a picture of the elephant’s tail – interesting but disembodied from the rest of the beast not that informative. As earlier commentators have noted, US MD’s are only part of the picture, as surrogates have increased their role in primary and surgical care. Even considering that, the picture painted is even more misleading. In California, for example, US educated MD’s account for only 50% of current, practicing physicians, the rest have gone to school in Canada or overseas, or are DO’s.
If you what to understand the physician pipeline, you have to look at residency slots as well (the allocation of which was part of what was sited for Roth’s Nobel). For example, shows a completely different picture. Note too that every year there are residency slots that are unfilled, (albeit in unpopular specialties). Expanding the number of US Medical school slots (two new medical schools here in California in the last 5 years) might mean fewer unfilled slots – and more primary care.
Then there is the whole issue of the subsidy system for academic medical centers, ostensibly to cover the cost of training physicians.
You missed an interesting consequence of the increase in what can be only viewed as the balancing of gender in medical school (considering that significantly more than 50 percent of college graduates are female); that is that female physicians work 6-7% fewer hours per week than their male counterparts (source: California MBCA database, March 2012). So the old physician to population ratios no longer work.
Zachary
Mar 4 2013 at 4:06pm
Micro fundamentals to the rescue!!
dave smith
Mar 4 2013 at 4:11pm
When my brother in law started Medical school, I went to his white coat ceremony, I expected the students to come from the most prestigious undergraduate institutions in the country. It turned out that almost all of them got their BA degrees from regional schools in the state where the medical school was. And almost every one of the was coated by a mother, father or uncle who was already a doctor…
So our doctors might be getting scarcer and dumber.
MingoV
Mar 4 2013 at 5:42pm
As I stated in a previous post, the federal government caused this. A federal government committee in the late 1970s came to the unwarranted conclusion that there were too many physicians in the USA. The actual problem was that there were too many physicians in cities with academic medical centers and too few physicians in rural and inner city areas. After reaching the wrong conclusion, the federal government used financial incentives to convince medical schools to keep class size fixed.
The next interference was in the 1990s when the federal government decided there were too many specialists and not enough doctors in family medicine, internal medicine, and pediatrics. Again, financial incentives were used on teaching hospitals to reduce specialty residencies and fellowships. The claim of too many specialists was based on a single study commissioned by Blue Shield that was misinterpreted. Medicine has become so complex that a generalist cannot keep up. We need more specialists, not fewer. For example, the elderly are the fastest growing age group in the country, but we have far too few geriatricians to care for them.
Highgamma
Mar 4 2013 at 6:09pm
Price of labor goes up. Capital is substituted for labor. Labor productivity rises.
If true, isn’t this a good thing?
ThomasH
Mar 4 2013 at 6:55pm
Did ACA or the Republican alternative provide more encouragement to the training of more doctors and to the use of alternative delivery models to reduce the demand for doctors?
Vincent
Mar 4 2013 at 9:12pm
Maybe they are much more efficient at delivering care.
Janine
Mar 4 2013 at 10:20pm
One problem with your conclusion- it is not that the federal government regulates the supply of doctors, it is that the federal government artifically caps the pay of most doctors- particularly “cognitive” and primary care doctors.
Our field has great deterrents to entry- large debt load, years of education and years spent in delayed gratification of basic lifestyle choices (like having children).
Young doctors have to sub-specialize (2-3 additional years of education) to get into technical one-organ fields that will pay back their debt.
Who would want to go into primary care medicine now? The working conditions have deteriorated every year for decades and the pay is lower now than when I graduated from medical school 20 years ago.
howard
Mar 4 2013 at 11:19pm
[Comment removed pending confirmation of email address. Email the webmaster@econlib.org to request restoring this comment. A valid email address is required to post comments on EconLog and EconTalk.–Econlib Ed.]
Jerome Bigge
Mar 5 2013 at 8:52pm
The AMA was organized back in 1846 with the express purpose of improving the status and income of doctors. Nothing wrong with that, we all organize ourselves for our own betterment. However the AMA used the power of government to establish a monopoly over the supply of medicine. In other words, the AMA used the force of government to gain its objectives. The other professions have done the same thing. This has resulted of course in much higher incomes for members of the professions, but this income can only be obtained by taking money from others using the force of government for the purpose. Without being able to use the force of government for this purpose, the incomes of professionals would be considerably lower than what it is. There would be no professional monopoly over access to medicine. The cost of health care would be much lower than it is today. Low enough that most people would not have a problem taking care of their own health for most of their own needs.
Comments are closed.